Cost-benefit analysis can increase trust in decision
makers
Jonathan Baron1
University of Pennsylvania, Andrea D.
Gurmankin
Rutgers University
Abstract
Four experiments on the World Wide Web asked whether people
trust an agent (a company or government agency) more when the
agent uses cost-benefit analysis (CBA) or, more generally,
bases decisions on their consequences. Experiment 1 used a
scenario concerning the installation of a safety device in a
car. The decision was made either by a company or a government
regulatory agency. Trust in the agent increased when the
decision made was consistent with the results of CBA. Part of
the CBA involved comparison with other safety devices that were
either installed or not. Such comparison increased trust even
when the subject disagreed with the agent's decision.
Experiment 2 replicated Experiment 1 with a health-care
scenario involving decisions by insurance companies about
whether to cover a treatment. Experiment 3 showed that trust
could be increased by CBA even in highly charged moral
contexts. Experiment 4 found that people are willing to take
cost into account more for social decisions than for individual
ones. The results together suggest that people might be
responsive to clear justifications of policies that emphasize
costs, benefits, and alternatives, even if these policies
violate their intuitions.
Introduction
Government regulatory agencies, courts, health insurers, and
other institutions sometimes try to adopt policies that bring
about the best overall outcomes, all things considered. In
trying to do this, they often use cost-benefit analysis (CBA) or
some other form of formal analysis based on the costs and
benefits of expected consequences. They may measure the
consequences in terms of money, life years, or utility. When
agencies (in this general sense) attempt to use CBA (likewise in
a general sense, including other forms of decision analysis),
they often face opposition, because people's intuitions are often
inconsistent with the results of CBA. If agencies are to succeed
in their efforts to improve outcomes, then people must trust the
agencies even when their policies are counter-intuitive. Can
people come to trust agencies that make decisions consistent with
CBA, despite the conflict with their intuition?
Breyer (1993) argues that regulation of risk is hampered by a
cycle in which the public reacts to some incident, such as Love
Canal (Kuran & Sunstein, 1999), the government passes some
poorly crafted legislation in response to public reaction, such
as the Superfund laws, and the legislation itself provokes a
counter-reaction, and the cycle continues. If the agencies were
trusted more, Breyer argues, the legislature would give them
broader scope, and they could regulate in the public interest.
In order to be trusted more, they must earn that trust: "Trust
in institutions arises not simply as a result of openness in
government, responses to local interest groups, or priorities
emphasized in the press - though these attitudes and actions
play an important role - but also from those institutions'
doing a difficult job well" (p. 81).
Breyer's solution is to develop, over time, a branch of the
bureaucracy that is in fact competent and expert in making
decisions according to their consequences and is also perceived
as being competent and expert. Bureaucrats in such a branch must
be competitively selected, well trained, and insulated from
outside pressure. Although Breyer does not mention it, the
current U.S. Federal Reserve may be a case in point (at least
until the next economic disaster). The control of interest rates
in the U.S. used to be heavily politicized, but now most citizens
(and legislators) seem to trust the Federal Reserve to try to
control interest rates in the public interest.
However, good decisions, that is, those that are in the public
interest, may not always be perceived as good decisions. Public
perceptions of risk seem to be influenced by intuitive judgments
that disagree with those that experts might make according to
CBA. Such intuitive judgments are often based on principles
other than those designed to bring about the best consequences.
Risk experts, of the sort that might serve in a Breyer-type
regulatory branch, are likely to be trained in welfare economics,
decision theory, and cost-effectiveness analysis. These
disciplines are based on theories about how to achieve the best
consequences (or why the best consequences are not achieved). In
the case of risk regulation, the best consequences amount to
minimizing harm for a fixed cost, or minimizing cost for a given
level of harm, or minimizing some weighted sum of cost and harm.
"Harm" may amount to something as simple as lost years of life
(or lost quality-adjusted years).
Currently, regulatory agencies, courts, and health-care providers
rarely rely on CBA. Thus, from the perspective of CBA, we could
do more good with less money than we are now doing. (See, for
example: Slovic, 1998; Tengs et al., 1995.) Psychological
research suggests that inefficient decisions of these agencies
are based to some extent on the nature of human judgments. On a
number of issues, people's intuitive judgments are biased
systematically away from the recommendations of CBA (Baron, 1998,
2000), such as the preference for harms of omission over harms of
commission. When acted on, such biases (away from maximization
of consequences) can cause worse outcomes. If we are concerned
with improving outcomes, then we might want to examine the role
of these effects in decision making.
As a result of such judgments, agencies are often put in a
conflict between the intuitions of their clients and the advice
of technical experts, who usually base their recommendations on
an analysis of consequences. This applies to such agencies as
the U.S. Food and Drug Administration (FDA) and the Environmental
Protection Administration (EPA). For example, EPA has recently
been taking into account the distribution of risk as well as its
total amount, thus siding with popular intuition. FDA may have
done the same in its recent decision to withdraw the rotavirus
vaccine. At an individual level, doctors who recommend DPT
vaccine are often caught in the same bind.
One way an agency might deal with such intuitions or biases is to
attempt to explain its actions, especially when they are
consistent with CBA but inconsistent with public opinion. Can
this help? The experiments reported here attempt to simulate the
effects of various types of CBA on trust.
Experiment 1
Viscusi (2000) asked juror-eligible citizens in the U.S. whether
they would assess punitive damages against a car company that
decided not to make safety improvements in a car's electrical
system, leading to deaths from burns, and, if they would assess
punitive damages, how much. When the company had carried out a
CBA to make the decision about making the safety improvements,
the proportion of subjects who assessed punitive damages was no
lower than when the company did not carry out the CBA (even
slightly higher). The analysis assigned a value to human life,
and raising this value up to $4,000,000 per life had no effect.
In fact, subjects assessed higher punitive damage awards when the
value of life was higher, apparently because they anchored on the
number given.
Viscusi's result is discouraging for the proponents of the use of
CBA by corporations and government. It suggests that when a
company uses such an analysis is used to justify inaction in a
case like this, it will make people no more forgiving of the
company.
Viscusi gave the scenarios with and without analysis to different
subjects. Such a between-subject design lacks statistical power,
and it may have missed detecting an effect even with several
hundred subjects. Of course, it did detect the anchoring effect
with the value of life, but that effect involved a numerical
response, and the main analysis was simply whether or not
punitive damages were assessed. The experiment may have been
insensitive because the probability of awarding some damages was
on the order or 90% overall, leaving little room for effects of
experimental manipulations.
Experiment 1 used a more sensitive design to assess responses to
CBA in the same context. It manipulated several variables
concerning the type of analysis done, and whether the final
decision is consistent with the analysis. It asked about trust
in the agency or company that did (or did not do) the CBA, and
about fines in case of injury. The fines serve as a second, more
concrete, measure of the extent to which the agency is at fault.
The general result is that, when the decision is consistent with
the analysis, CBA increases trust and reduces fines assigned for
mishaps, regardless of whether the decision suggested by CBA is
consistent with the subject's judgment.
Method
Ninety-five subjects completed a questionnaire on the World Wide
Web. Their ages ranged from 18 to 74 (median 34); 26% were
male; 9% were students. The questionnaire began:
Safety features
This questionnaire concerns the trade-off between money and
safety. Governments and corporations are faced with choices, in
which they can spend more money and reduce risk.
The safety issues concern prevention of injuries and death.
We shall give the number of "serious injuries" in each case. All
serious injuries require hospitalization. Half of these injuries
result in some permanent disability, and 10% result in death.
The cost of prevention is paid by consumers. For example, if
a safety device is put in a car, the price of the car increases
by the cost of the device.
The questions ask what you would do in such cases, and also
how much you would trust government agencies or corporations that
made various choices.
Some items ask you to compare two government agencies,
concerned with safety regulation. Imagine that either of these
agencies could make a regulation about the device in question.
Also, imagine that these agencies could be sued in court, just as
corporations can be sued.
We are interested in what reasons you think are relevant to
these decisions, so please pay attention to the different
reasons.
Each screen involved a comparison of two agents (corporations or
agencies). The first agent always based the decision on cost
alone. The second agent based the decision on benefit as well as
cost (although the decision was the same). On half of the cases,
the second agent also compared the device in question to other
devices. The wording read, with alternatives and noted in
brackets:
Consider a safety device for cars. Its cost is $50
per car, and it would increase the car's price by $50. Its
benefit is that it would prevent 50 [5]
serious injuries, for 200,000 drivers. It would reduce each
driver's chance of injury by .025 [.0025] % over the lifetime
of the car.
Other safety features not [now] installed in cars
could prevent injuries at a lower [higher] cost per
injury prevented.
Should the government require [Should a company install] the
device?
Agency [or Company, throughout] A decided [not] to require that
the device be installed [install the device]. Agency A knew the
cost of the device, but it did not try to discover the benefit
of the device (the number of serious injuries prevented, which
you were told above). Agency A based its decision on cost
alone.
Agency B also decided [not] to require that the device be
installed [install the device]. Agency B did discover the
benefit (the number of serious injuries prevented) as well as
the cost. Agency B based its decision on the average cost of
preventing each serious injury.
Agency B did not attempt to compare the costs and benefits of
this device to other safety features already installed in cars
that prevent injuries at a higher or lower cost per injury
prevented.
[For half of the cases, the last two sentences were:] Agency B
also determined that other safety features [not] installed in
cars can prevent injuries at a higher [lower] cost per
injury prevented.
Which agency would you trust more to make decisions like this
in the future?
[If the device was not installed, the following was asked:]
Suppose both agencies were sued in court because they did not
require that the device be installed. Injuries occurred that the
device would have prevented. The law says that the maximum
payment to victims is $1,000,000 per injury. How much should
each Agency pay each victim (in thousands of dollars, digits only)?
Agency A $ Agency B $
The 32 screens were presented in a different random order for
each subject. Each screen described two agents (decision
makers). The 32 screens represented all possible combinations of
two levels of each of five variables:
- Government agency vs. private company as the agent
(manipulated mainly to increase the number of cases per subject);
- Benefit of the safety device (5 vs. 50 serious injuries);
- Whether the device was to be installed or not (the same for
both agencies);
- Whether the device had a higher cost-effectiveness than other
devices now installed vs. a lower cost-effectiveness than
other devices not installed (betterness);
- Whether the second agent had determined #4 or not
(knowledge).
Note that #4 implied either that the device was probably worth
installing, since it was more cost-effective than other devices
installed, or that it was not worth installing, because it would
be more cost-effective to install some other device. Thus, this
manipulation put the decision in a larger context, as a more
thorough CBA would do.
Results
Because the design was within-subject, all analyses are based on
t tests of contrasts or interactions (differences of differences).
Whether the device should be installed
Consider first the question about whether the device should be
installed (Should-install). On the average, subjects favored the
installation of the device, with a mean score of 0.31 (which
differs from 0; t94=5.11, p=.0000) on a scale where 0 is
neutrality and each step on the answer scale is 1 unit (so that
"probably" is .50, and "certainly not" is -1.5).
Should-install was sensitive to the benefit (.45 with 50
injuries, .17 with 5; t=6.55, p=.0000), although 47% of the
subjects showed either no effect or a (small) reversed effect.
(Some of this 47% favored the device very strongly regardless of
the benefits.)
Should-install was also sensitive to the implications of
comparisons to devices installed or not installed (.58 when less
cost-effective devices installed, .05 when more cost-effective
devices not installed; t=6.92, p=.0000; 31% showing no
effect or a small reversal). Call this the effect of
"betterness."2
Trust
We ask two questions about trust. First, do people trust the
agent that considers both benefit and cost (B) more than the
agent that considers only cost (A)? This is the simplest
question about whether CBA increases trust. Second, is trust
affected by whether B act's consistently with the results of the
analysis?
On the first question, Table shows the means for
trust in the agent that did the more thorough analysis (B).
Agent B examined both benefits and cost while agent (A) examined
only cost. The two agents on each screen always made the same
decision. The fact that these numbers are positive indicates
that subjects were more inclined to trust the more thorough agent
(B); the mean rating was .68 on a scale where each step is 1 unit
and 0 is neutrality (t=13.03, p=.0000).3
Table 1: Trust in B, the more thorough agent (0 is neutrality).
| Not installed | Installed |
| No knowledge | Knowledge | No knowledge | Knowledge |
| 5 lives, worse | 0.43 | 0.85 | 0.62 | 0.77 |
| 50 lives, worse | 0.43 | 0.82 | 0.73 | 0.79 |
| 5 lives, better | 0.46 | 0.53 | 0.62 | 1.03 |
| 50 lives, better | 0.39 | 0.48 | 0.75 | 1.13 |
Turning to the second question, about consistent action, the size
of the benefit (number of lives saved) should affect the
desirability of installing the device and should thus interact
with whether the device is installed. B should be more trusted
when B is responsive to benefit. Although size of the benefit
did not have a significant main effect, higher benefit leads to
more trust when the device is installed than when it is not
installed (t=2.71, p=.0079).
Betterness - whether the device was better (in
cost-effectiveness) than installed devices vs. worse than
uninstalled ones - also had no main effect. Betterness should
increase trust when B knows about it and acts on it. Thus, it
should interact with knowledge and installation.
Knowledge - whether the agency knew about betterness -
increased trust (t=7.09, p=.0000). Knowledge did not
interact with installation, betterness, or benefit. However the
expected triple interaction between knowledge, betterness, and
installation was significant (t=5.66, p=.0000). Knowledge
led to the highest trust when the device was better than other
devices and when it was installed (lower right of Table
1). When the device was better and not installed,
knowledge did not affect trust significantly either way.
Importantly, though, knowledge led to increased trust when the
device was worse and was not installed (the upper left of the
table; t=7.62, p=.0000). In sum, the agency earned more
trust when they attended to comparative information and followed
its implications.
In sum, knowledge about betterness increase trust in decisions
that are consistent with that knowledge. Does this effect happen
even when the subject disagrees with the agency's decision? To
test this, we examined pairs of cases (screens) that differed
only in knowledge. We selected those pairs in which the subject
disagreed with the agency's decisions in both cases. (25 subjects
had no such pairs.) Knowledge led to greater trust even within
these pairs (mean effect of 0.34, t69=5.04, p=0.0000).
Fines
In cases where the agency or company described did not install
the device, we asked about fines (with a maximum of $1,000,000
per injury). The mean fine for agent A (no analysis of benefit)
was $504,000, and the mean for B was $440,000. The range of
fines was high, however. To get a better measure of the relative
fines for A and B, we computed the ratio 2A/(A+B)-1, which
would be 1 if the subject fined agent A and did not fine B, -1
if the subject fined B but not A, and 0 if the fines were equal.
(Fines of 0 for both were treated as missing data.) The mean of
this measure, 0.098, was positive (t93=5.00, p=.0000),
indicating that more analysis led to lower
fines.4
Table shows how this measure depended on
knowledge, benefit, and betterness. Recall that the measure is
higher when agent B, the one who does more analysis, is fined
less for not installing the device. It is thus parallel to the
measure of trust in B, when B does not install the device.
Table 2: Relative fine for A (no analysis) vs. B (1 if all for
A, -1 if all B).
| No knowledge | Knowledge |
| 5 lives, worse | 0.101 | 0.162 |
| 50 lives, worse | 0.066 | 0.173 |
| 5 lives, better | 0.071 | 0.069 |
| 50 lives, better | 0.099 | 0.048 |
The measure was higher (B fined less) when the uninstalled device
was worse compared to the alternatives (t = 3.71, p = 0.0004), when it had less benefit (t = 1.85, p = 0.0677),
and when B had knowledge of this (right column vs. left, t = 4.12, p = .0001).
Of greater interest is the interaction between knowledge and
betterness (t93=3.17, p=0.0021). The effect of betterness
(top two rows vs. bottom two rows in Table 2) was
greatest when B was informed about it.5 In sum, appropriate use
of CBA reduces fines. The results parallel those for the trust
measure.
Does the effect work with all subjects?
It is possible that - despite the main effect of increased
trust in those who use CBA - some subjects distrust CBA so much
that it reduces their trust. Clearly this did not happen with
most of our subjects, as the overall effect was to increase
trust. To examine individual differences, we carried out a
one-tailed t test for each subject in "trust in agent B." The
test was one tailed because we were looking only for subjects who
trusted B less than A. But, of course, with enough subjects,
some of these tests would be significant by chance alone. Thus,
we examined adjusted p-levels for multiple tests. We used the
step-down resampling procedure of Westfall and Young (1993) as
implemented by Dudoit and Ge (2003). By this test, 2 subjects
showed significantly greater trust in agent A at p < .05 (one
tailed - p=.0223 for both). Thus, CBA reduces trust for some
people, but not for very many in our population.
Experiment 2: Health insurance
Experiment 2 replicated Experiment 1 in the context of health
insurance.
Method
One hundred and two subjects completed a questionnaire on the
World Wide Web. Their ages ranged from 18 to 74 (median 35);
28% were male; 15% were students. The questionnaire began:
Health insurance
This questionnaire concerns the trade-off between money and
health. Health insurance companies must decide which treatments
to cover (pay for).
On each screen, you will see some information about a cure for
a serious disease. Suppose that all diseases are quite serious
and chronic, making for a low quality of life and usually a
shorter life too. Examples are diseases like severe arthritis,
senility, emphysema, and heart disease.
The treatments work with one type of each disease, so they are
given only to people with that type. Once the patient is
diagnosed as having that type of disease, the treatment is given
all in one dose of a drug. The drugs are expensive because of
the methods needed to produce them.
You will see:
- The number of people who have the type of disease and can get
the treatment.
- The percent of these that will be cured (100% or 50%).
- The cost per treatment.
- The increase in the insurance premium required to pay for
this coverage. The total cost of the treatment must be divided
up among 10,000,000 policy holders.
- The cost per cure (the same as the cost per
treatment when the cure rate is 100%).
- A comparison of the cost per cure with other treatments that
are currently covered or not covered.
You will also see information about two different insurance
companies and how they decided whether or not to cover the
treatment. We are interested in what reasons you think are
relevant to these decisions, so please pay attention to the
different reasons.
You will be asked
- Whether the treatment should be covered.
- Whether you would trust each insurance
company to make future decisions of this sort.
- Which company you trust more.
The wording of the items read [with alternatives in brackets]:
- This type of disease affects 1,000 [2,000] people per year.
- The treatment would cure 1000 of these people, or 100%
[50%] of them.
- The cost per treatment is $200,000 [$2,000,000].
- If this treatment is covered, the annual premium paid by
each of the 10,000,000 policy holders must increase by $20 [$40, $200, $400].
- Because the treatment cures 100% [50%]
of those who get it, the cost per cure is
$200,000 [$400,000, $2,000,000, $4,000,000].
- Other treatments not [currently] covered by Companies
A and B could cure more [less] serious diseases at a
lower [higher] cost per cure.
Should insurance companies cover the treatment?
Company A decided [not] to cover the treatment. Company A knew
the cost of the treatment for each policy, but it did not try
to discover the benefit of the treatment (the percent of cures,
which you were told above). Company A based its decision on
cost alone.
Company B also decided [not] to cover the treatment. Company B
did discover the benefit (the percent of cures) as well as the
cost.
Company B based its decision on the cost per cure. Company B
did not attempt to compare the costs and benefits of this
treatment to other treatments that it currently covered or did
not cover.
[Company B also determined that other treatments that it
did NOT cover currently [currently covered] could cure more
[less] serious diseases at a LOWER [HIGHER] cost per cure.]
On the basis of this information alone, how would
you feel about having insurance from Company A
On the basis of this information alone, how would
you feel about having insurance from Company B
Which company would you trust more to
make decisions like this in the future?
Each subject saw all combinations of the five variables in a
different random order. The variables were: Cost, Cure rate,
Coverage (whether A and B covered the treatment or not), Better
(whether the treatment was better than alternatives in terms of
cost and effectiveness, or worse in terms of both), Compare
(whether the company compared the option to alternatives). The
premium increase was derived from Cost and Cure rate.
Results
In general, subjects favor decisions that are consistent with a
CBA. The measure Should-cover, the subject's opinion about
whether coverage should be offered, was defined so that 0 was
neutrality and each step on the scale was one unit. The means of
Should-cover depended on Cure (.65 for 100%, .11 for 50%), Cost
(.02 for high cost, .65 for low), and Better (.52 for Better, .16
for Worse). All differences were highly significant (p=.0000),
and no interaction was significant.
Table shows the means for Feelsum, the sum of the
two measures of how the subject felt about the two companies.
Both made the same decision, so this serves as an overall measure
of confidence in that decision. All of the first-order
interactions shown were highly significant (p=.0000): subjects
favored coverage more (larger difference between Not cover and
Cover) when the treatment was lower cost, when it cured 100%,
and when it was the Better option. No higher-order interaction
was significant.
Table 3: Means for Feelsum, the sum of how subjects felt about
the decision, as a function of cost, coverage, benefit and
betterness.
| Not cover | Cover |
| High cost | -0.45 | -0.24 |
| Low cost | -1.13 | 0.59 |
| 50% cure | -0.61 | -0.04 |
| 100% cure | -0.98 | 0.39 |
| Worse | -0.51 | -0.15 |
| Better | -1.07 | 0.50 |
Table shows the results for the questions about
how the subjects would feel about getting insurance from the two
companies, coded so that positive numbers represent better
feelings about B (the more thorough company). Here we could also
assess the interaction of Cost, Cure and Betterness with
Coverage. The interaction between Cost and Cover was significant
(t101=2.55, p=0.0122), as was that between Better and
Cover (t101=4.87, p=0.0000), but the interaction between
Cure and Cover was not significant. In general, though, people
feel better about B, the more thorough company, when it is
responsive to Cost and Betterness.
There was also a triple interaction between Betterness,
Comparing, and Coverage (t101=5.89, p=0.0000). This is
what we would expect if the increased trust resulting from
responsiveness to Betterness were found mainly when Company B
made the comparison so that it knew about Betterness. In other
words, Betterness affects trust only when Company B took the
trouble to find out about betterness.
Table 4: Differences in feeling about Company A and B, with
positive numbers indicating better feeling about B (the more
thorough company).
| Not compare | Compare |
| Not cover | Cover | Not cover | Cover |
| High cost | 0.17 | 0.27 | 0.45 | 0.53 |
| Low cost | 0.17 | 0.30 | 0.38 | 0.65 |
| 50% cure | 0.16 | 0.29 | 0.45 | 0.55 |
| 100% cure | 0.19 | 0.28 | 0.38 | 0.63 |
| Worse | 0.17 | 0.30 | 0.69 | 0.45 |
| Better | 0.18 | 0.27 | 0.14 | 0.73 |
Table shows a parallel analysis for Trust, the
question about whether the subject would trust B more than A. In
this case, the interactions with Coverage were all significant:
Cost (t101=3.61, p=0.0005); Cure (t101=2.13,
p=0.0353); and Better (t101=4.87, p=0.0000). Again, the
triple interaction between Betterness, Comparison, and Coverage
was significant (t101=6.53, p=0.0000).
Table 5: Differences in trust in Company A and B, with
positive numbers indicating more trust for B (the more
thorough company).
| Not compare | Compare |
| Not cover | Cover | Not cover | Cover |
| High cost | 0.22 | 0.26 | 0.42 | 0.49 |
| Low cost | 0.18 | 0.34 | 0.38 | 0.65 |
| 50% cure | 0.18 | 0.28 | 0.43 | 0.50 |
| 100% cure | 0.22 | 0.31 | 0.38 | 0.64 |
| Worse | 0.19 | 0.29 | 0.66 | 0.42 |
| Better | 0.21 | 0.31 | 0.14 | 0.72 |
Again, the main results so far are consistent with the general
conclusion that trust increases when the decision maker adopts a
strategy of doing thorough analysis and following its
conclusions. Again, we asked whether such a strategy is
effective even when the subject disagrees with the decision to
which it leads, which was the same for both companies in each
case. Knowledge increased trust in Company B (the more thorough
company) when the decision was consistent with betterness (better
and covered, worse and not covered) even on just those pairs of
cases in which the subject disagreed with the agent's decision in
both cases in the pair (mean effect of 0.27, t84=3.66,
p=0.0004).
In this study, 6 subjects (6%) were significantly more trusting
of the company that did less analysis (A), after
correcting for multiple tests as in Experiment 1. As in
Experiment 1, the attempt to use the results of CBA in the
context of health coverage can actually reduce trust for some
people. The number is small enough, however, so that it seems
unlikely to become a majority even with a different method of
sampling.6
Experiment 3
The present experiment examines the effect of CBA on trust in a
more morally charged context. Subjects were presented with items
found in other studies to be morally objectionable even though
they might conceivably lead to good outcomes, such as cloning.
Many people think that cloning (for example) should be completely
prohibited. We asked whether they could trust a government agency
that would not prohibit it, if a CBA indicated that cloning was
useful in some cases. Of course, a demonstration that a
procedure is sometimes useful does not necessarily imply that an
agency could craft a rule that would permit it when it was useful
and prohibit it otherwise, but such a demonstration would provide
some justification for not banning the procedure totally. Are
people responsive to such a justification?
Method
One hundred and five subjects completed a questionnaire on the
World Wide Web. Their ages ranged from 20 to 74 (median 38);
27% were male; 13% were students. The questionnaire began:
Medical procedures
This questionnaire concerns some medical procedures that have
been much in the news recently, such as cloning. One issue is
whether qualified doctors should be allowed to do them if
patients want them.
Please assume that all of these procedures have been perfected so
that they are completely safe and have their intended
effect.
[There were then some brief definitions of terms used in the
cases: artificial insemination, cloning, in-vitro fertilization,
embryonic stem cells, Alzheimer's disease, prenatal genetic
testing, spina bifida.]
Many people object to procedures like cloning or abortion on
moral grounds. Note that you can object to a procedure on moral
grounds and still think that someone might benefit from it. Some
questions may require you to imagine this kind of conflict
situation.
Each item began with one of the following 16 procedures (the
numbers in brackets are mean responses to ALLOW, TRUST, and CBA
questions, respectively, as explained later).
- giving a drug to cause death in a terminally-ill patient with
un-treatable pain, who requested the drug, and who was judged to be
rational by two doctors [0.68, 0.52, 0.56]
- giving a drug (with no side effects) to enhance school performance
of normal children [-0.18, -0.30, -0.18]
- transplanting the organs of a person who left no record
(either written or verbal) of his willingness or unwillingness
to be an organ donor, in order to save the life of someone who
needed an organ [0.47, 0.41, 0.52]
- cloning an adult human, who had difficulty having a child,
to produce a child who would be raised by the adult [-0.16, -0.20, -0.18]
- cloning an adult human to produce a fetus, which would be
aborted and used for cells to save the adult's life [-0.09, -0.22, -0.18]
- cloning an adult human to produce a fetus, which would provide
cells to save the adult's life and which would then be born
and raised as the adult's child [0.16, 0.09, 0.16]
- using in-vitro fertilization to produce stem cells for
treatment of Alzheimer's disease [0.62, 0.35, 0.43]
- having a child because, after birth, it could be a bone-marrow
donor and save the life of another child [0.68, 0.49, 0.56]
- testing a fetus for sex and aborting it if it is a girl
[-0.87, -0.60, -0.64]
- testing a fetus for spina bifida and aborting it if it has
spina bifida [0.60, 0.37, 0.39]
- testing a fetus for IQ genes and aborting it if its expected IQ
is below average [-0.73, -0.62, -0.58]
- modifying the genes of an embryo so that, when it is born, it
will have a higher IQ [-0.45, -0.43, -0.35]
- cloning someone with desired traits so that these may be
passed on, such as an athletic champion or brilliant scientist
[-0.50, -0.50, -0.41]
- using in-vitro fertilization to have one's own child [0.85, 0.70, 0.77]
- using in-vitro fertilization and then having the egg implanted in
another (surrogate) woman, who would give up the baby at birth
[0.81, 0.71, 0.77]
- using artificial insemination to have a child with a desired trait,
by choosing a donor with this trait, such as intelligence [0.37, 0.24, 0.26
The items were presented in a random order chosen separately for
each subject, twice (in the same order for each subject - so
that some questions were maximally far apart). The subject
answered 4 questions in the first pass and five in the second
pass. Here I present only the questions relevant to this article
(ALLOW in the first pass, the others in the second):
ALLOW. Should the government allow this procedure? [Response options:
This should be allowed, so long as other laws are followed. This
should sometimes be allowed, with safeguards against abuse. This
should never be allowed, no matter how great the need.]
TRUST. Suppose two government agencies could have the power to decide
which medical procedures are prohibited. The two agencies are
similar, but agency P would prohibit this procedure completely
and agency N would not. Which agency would you trust more to
have the power to decide? [P; N]
CBA. Suppose that a team of economists and other
researchers did an analysis of the effect of allowing this
procedure under certain circumstances. The team reported that
the procedure could do some good in these circumstances, and
nobody would be harmed. In this case, which agency would you
then think should have the power to decide about prohibition?
Remember, agency P would prohibit this procedure and agency N
would not. [P; N]
Results
The mean answers to the ALLOW, TRUST, and CBA questions for each
item are shown above in brackets, respectively. ALLOW was scored
so that 1 favored allowing and -1 favored prohibition (with 0
representing "sometimes"). TRUST and CBA were scored so that 1
represented N (not prohibit) and -1 represented P (prohibit).
The main result was that CBA responses (empowerment after the CBA
showed benefit) were higher than TRUST responses (before the CBA;
t104=4.17, p=0.0001; the result was also in the same
direction for all but one of the items). In sum, subjects were
more willing to trust - i.e., give power to - an agency that
would allow the procedure when they were told that the a CBA had
shown that the procedure could be beneficial on the whole.
Again, we asked whether any subjects showed significantly less
trust with CBA than without it, the opposite result from that
just reported. In this case, no subject showed a significant
reversal.
Experiment 4: efficiency for social vs. individual
decisions
CBA is often criticized for being concerned with efficiency at
the expense of individual welfare. In the trade-off between cost
and benefit of medical treatments, for example, people may think
that they should get an effective treatment even if it is
extremely expensive. Yet many agencies want to impose some sort
of rationing based on CBA, and such rationing has been found to
strike many as unfair or immoral (Ubel, 2000). If people want
agencies to follow their individual preferences, they will oppose
any effort to ration expensive treatment. If, on the other hand,
people accept the need for rationing at a societal level, they
may tolerate it as a matter of policy, even if they would not
want it for themselves.
The last experiment compared decisions about the self to two
types of policy decisions: decisions about voting, and decisions
about which agency to trust. We hypothesized that self decisions
would favor greater benefit at the expense of greater cost,
compared to the two societal level decisions.
Note that this is not necessarily a matter of selfishness,
although it may appear that way to the subjects. When treatments
are provided by government or by insurers, someone must pay for
them, and the payers are ultimately the same people as those who
might need the treatment (at least over a range of treatments -
e.g., women do not get testicular cancer, but they do get breast
cancer more than men do). The situations described were
sufficiently general so that subjects had no good reason to think
that they would benefit more than would others, or pay less than
others, from a decision to provide an expensive treatment.
Likewise, acceptance of rationing would not make people less
altruistic, in a formal sense. Instead, true altruism would
consider both the health benefits and costs for others. If
people thought that others were like themselves, perfect altruism
would lead to the same preferences for self and others. Subjects
in this experiment are asked to assume that they are
typical.7 If subjects are more inclined to choose
cost-effectiveness in policy than for themselves, we can think of
this (formally described) as a kind of differential altruism, in
which they express more concern for others' finances than for
others' health, relative to what they want for themselves.
We hypothesize, however, that people will think differently about
the individual case because of the "identifiable victim effect"
(Jenni & Loewenstein, 1997; see also Baron, 1997, for a related
result). They tend to think of the benefit to individuals,
themselves, as solving a single problem, that of the individual,
with the cost spread over millions of people, each of whom does
not notice the difference.
Alternatively, the same result could arise from a kind of
misguided selfishness, in which people mistakenly think about the
benefit and not the cost when thinking about themselves, even
though the social decision involves the identical trade-off, on
the average, for everyone. Our experiment does not distinguish
these explanations, but it does show that people may accept
rationing by CBA at a policy level even when they oppose its
implications for themselves.
Method
One hundred and seventy-eight subjects completed the questionnaire
(ages 18-67, median 38); 30% were male; and 12% were students.
Treatments
This questionnaire concerns decisions about medical treatments
for one-time epidemics of new infectious diseases. The question
is what to do if the epidemic hits.
The diseases in question all have fatality rates of 10%. Each
disease will affect 1% of the population, without regard to age,
sex, race, or health status.
Nothing can be done to prevent infection. Everyone is equally at
risk. Thus, each person has a 1/1000 chance of death, unless
treatment is available.
There are 32 screens, each with 4 questions. Some screens may
look the same as others. They are not. The numbers are different.
Please pay attention to the numbers.
Some questions concern your own choices for yourself, and others
concern your nation. Imagine that you are typical of your nation
in terms of your ability to pay.
One question concerns the relative strengths of two arguments. I
am interested in cases where the relevance of an argument depends
on the kind of decision you are making. For example, some
arguments may be more relevant to decisions about yourself, or
other arguments may be more relevant to decisions about your
nation. Please read these carefully.
Suppose that your nation has both private health insurance and
government coverage for at least some treatments. Some questions
concern private insurance, and others concern government payment.
[Here is an example of an item:]
Reminders:
- Each person has a 1% chance of infection.
- 10% of those infected will die.
- An 'effective treatment' cures the infection and thus cuts
the chance of death in those infected by 10%.
- Treatments that cost more than $4,000,000 per life saved
are usually considered too expensive.
The government will pay for the treatment for all who get the disease.
Treatment X cures 100% at a cost of $50,000 per case treated -
$5,000,000 per life saved. The source of the money will be
determined later.
Treatment Y cures 50% at a cost of $8,000 per case treated -
$1,600,000 per life saved. The source of the money will be
determined later.
[Subjects did not see the names of the questions]
1. [Vote] Suppose the national government had to decide on X or Y, and
it has a vote (as part of another election). Which would you vote
for? ('Equal' means that you would abstain on this question.) [X
Y Equal]
2. [Trust] Suppose that two candidates in this national election argue
for different treatments.
Candidate X argues for X because it cures the most people.
Y argues for Y because it is the most cost effective.
Based on this information alone, which candidate would you trust
the most to make decisions like this in the future (on his/her
own)?
3. [Self] How would you choose between X and Y for yourself? (Suppose
you are typical of those affected in questions 1 and 2, in your
ability to pay.)
[The treatments were repeated as a reminder.]
4. Note that treatment X cures the most people, and treatment Y
is the most cost effective. Consider the relative strength of
these arguments.
Which argument is more relevant to each type of decision?
- CURES THE MOST PEOPLE is more relevant to deciding for myself,
and/or IS THE MOST COST EFFECTIVE is more relevant to what I
support for my nation.
- CURES THE MOST PEOPLE is more relevant to what I support for my
nation, and/or IS THE MOST COST EFFECTIVE is more relevant to
deciding for myself.
- The arguments do not differ in either of these ways.
The 32 items varied in whether the method of payment was
determined later (as in the example) or paid by those affected,
in which case the item read, "Your taxes [insurance premium]
will increase by [the cost per case treated divided by 100] for
one year." The purpose of this variation was to test the
hypothesis that people would be more willing to pay for something
when the source of the payment was unspecified. Otherwise, we
wanted to make clear that those who might need the treatment
would collectively pay for it, one way or another.
The items also varied in whether the treatment was provided by
government or insurance, and, orthogonally, in the cost of
Treatment X, the high-cost condition, which was either $50,000
(as in the example above) or $100,000 per treatment. (The
low-cost condition cost was always $8,000.)
Finally, there were four different price conditions, included
largely to create variation so that we could collect more data
from each subject:
- The high-cost treatment was 100% successful and the
low-cost treatment was 50% successful.
- 50% and 25% success, respectively, with the cost of each
treatment divided by two so that the cost per life saved was
the same as in condition 1.
- 100% and 25%, respectively, with the cost of the low-cost
treatment divided by two, again holding constant the cost per
life saved.
- The same as condition 1, but with all costs divided by 10
(so that even the high-cost treatment was within the usual
accepted range).
Results
Figure shows the proportion of responses of each
type - favoring the expensive treatment (X), favoring the
efficient treatment (Y), equal - as a function of the question.
The main result is that, as hypothesized, the Trust question
(Which candidate would you trust?) and the Vote question (Which
treatment would you vote for?) each yielded more support for
efficiency than did the Self question (Which treatment would you
choose for yourself?). When responses were coded as 1 for
expensive and -1 for efficient, and the mean for each subject was
computed for the 32 questions, Self was higher than Vote
(t177=5.02, p=0.0000), and Self was higher than Trust
(t177=3.00, p=0.0031). (The Vote-Trust difference was
also significant, but we had no hypothesis about it.) In sum,
people were more accepting of efficiency considerations for
policy than for themselves.
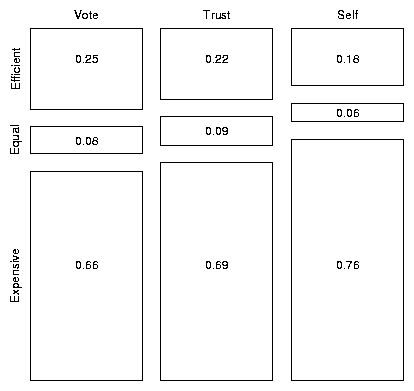 Figure 1: Proportion of responses of each type as a function of
the question.
Figure 1: Proportion of responses of each type as a function of
the question.
These results were equally strong (and both significant) when the
case involved payment as when the source of funding was
unspecified. (The interactions with pay were approximately
zero.) In the pay condition, the cost to the taxpayer or policy
holder was the same, and specified, for all questions. We do not
take this lack of effect as a definitive refutation of the
hypothesis that people are more willing to demand costly policies
when the source of payment is unspecified. Rather, the
within-subject design may have led subjects to realize that,
indeed, someone has to pay.
Some subjects showed the reverse effects. The self-trust
difference was significantly negative (less expensive favored
more in the question about self than trust in an agency) for 7%
of the subjects. The same percentage showed a reversed effect
for the self-vote difference. Possibly these subjects did not
want to withhold an expensive treatment from others out of
stinginess about paying for it, even though they would be
unwilling to pay for it (through insurance) for themselves.
Question 4 concerned the relative strength of arguments about
cure rates and cost-effectiveness. On the average, more
responses indicated that the cure-rate argument was more relevant
to the self and the cost-effectiveness argument was more relevant
to the government than the reverse (t177=5.45, p=0.0000,
across subjects). (Three subjects, in comments, said they had
trouble understanding this question.) 55% of the subjects
showed a significant positive effect (cure-rate more relevant to
self) and 21% showed a significant reverse effect. The mean
response to Question 4 correlated .34 (p=.0000) with the
self-vote difference.
The different attitude toward the self was reflected in several
comments. Here are two of the longer ones: "Most all of my
answers were the same here. The reason for this was because when
deciding for myself, I will always choose the moral decision of
deciding to save the most lives. When it comes to putting some
one in charge of making the decisions for me, I feel that the
person making the cost effective choice is the best for the
economy. Although saving lives seems to be the most ethical, if
we have medical expenses rise that much, our budget will all be
out of whack." "I think anytime we can cure more people it
should be done unless determined too expensive is my view for
nation. As for myself I will always want the one that cures the
most, it may be bad to look at it that way but I suppose it's
like running a business with the nation and with myself there is
no room for debate. I want the one that cures the most
regardless."
Twenty percent of the subjects consistently chose the more
expensive treatment in all conditions. Typical of their comments
was, "I would not consider cost effectiveness when trying to
save lives." No subject consistently chose the more
cost-effective treatment.
The different cure-rate/price conditions were included mainly to
get more data and to create conditions that might lead to
within-subject variability. However, one result of interest was
that the expensive treatment was chosen more often in the third
conditions, with cure rates of 100% for the expensive treatment
vs. 25% for the efficient one, than in either of the first two
conditions (100% vs. 50%, 50% vs. 25%). Averaging across
all three measures (Vote, Self, Trust), the mean responses (with
1 favoring the expensive treatment) were .33, .32, .54, and .75,
for the four cure-rate/price conditions, respectively. The third
was significantly greater than either of the first two at
p=.0000 by t test for every comparison. Subjects seem to be
influenced by the large difference in cure rate, even though it
is balanced by a large difference in cost. The fourth condition
represented a lower cost for all treatments, and the responses
were higher than those of all other conditions, as they should be
by any account.
Conclusion
The results of Experiments 1 and 2 support the view that CBA,
when it involves comparison to alternatives and when its results
are acted upon, can increase trust in decisions. Although
Viscusi (2000) suggested the opposite, his results were weak
statistically, and many of them were limited to the very few
subjects who were least inclined to award punitive damages, as
almost all of his subjects did award such damages in all
conditions, leaving little room for any effects. In addition, as
Viscusi points out, the sizes of damage awards in his study may
have been larger with a larger value of life because subjects
anchored on the value when determining their award. The present
within-subject design apparently reduced such an anchoring
effect, so that the benefits of CBA could be seen.
Of interest in these experiments is that CBA increased trust even
when the subject disagreed with its conclusion. Thus, CBA can
apparently help win trust even among those who disagree with the
policy that is adopted, provided that people are adequately
informed about the basic reasoning behind the CBA.
Experiment 3 showed that trust could be increased by CBA, even in
highly charged moral contexts.
Experiment 4 found that people accept rationing on the basis of
cost more for social decisions than for individual ones. It is
not clear here which option is the true optimum in terms of
utility. (Health and life may be worth more than people are
willing to pay for them at a societal level.) People may feel
that their own life is worth more than the lives of others, but
the insurance context of the experiment implies that they would
be paying for others anyway. If they truly understand that
insurance implies that everyone pays and everyone (potentially)
benefits, then we could take their Self judgments as being
"real." People may not fully understand, however. When they
answer about themselves, they may focus on the idea that one
person is benefiting while everyone is paying. And they may
think, "For myself, cost is no object," without realizing that
their endorsement of this view implies the same for everyone.
It is also not clear whether CBA in general, properly done,
favors more spending or less on health care than is now spent,
but at some point CBA will limit spending. The experiment
indicates that people are willing to take cost into account, as
well as benefits, when evaluating a policy that affects many
people.
The use of a within-subject design had the main purpose of
increasing the statistical power of these studies, but it may
also have been unrealistic. Arguably, some decisions are made
without any comparison, such as the assignment of punitive
damages in legal cases. On the other hand, other real cases may
be modeled better by a within-subject design, such as a change in
policy. When an agency or company announces that it is going to
start doing CBA, people will naturally evaluate this change by
comparing the situation before the change with the situation
after it. Our results suggest that people will, in general,
perceive the adoption of CBA as a good thing.
References
Babcock, L., Gelfand, M., Small, D., & Stayn, H. (2003). The
propensity to initiate negotiations: toward a broader
understanding of negotiation behavior. Under review.
Baron, J. (1995). Blind justice: Fairness to groups and the
do-no-harm principle. Journal of Behavioral Decision
Making, 8, 71-83.
Baron, J. (1997). Confusion of relative and absolute risk in
valuation. Journal of Risk and Uncertainty, 14, 301-309.
Baron, J. (1998). Judgment misguided: Intuition and
error in public decision making. New York: Oxford University
Press.
Baron, J. (2000). Thinking and deciding (3rd edition).
New York: Cambridge University Press.
Breyer, S. (1993). Breaking the vicious circle: Toward
effective risk regulation. Cambridge, MA: Harvard University
Press.
Dudoit, S., & Ge, Y. (2003). Bioconductor R packages for
multiple hypothesis testing: multtest.
http://www.bioconductor.org.
Jenni, K. E., & Loewenstein, G. (1997). Explaining
the"identifiable victim effect." Journal of Risk and
Uncertainty, 14, 235-257.
Kuran, T., & Sunstein, C. R. (1999). Availability cascades and
risk regulation. Stanford Law Review, 51, 683-768.
McDaniels, T. L. (1988). Comparing expressed and revealed
preferences for risk reduction: Different hazards and question
frames. Risk Analysis, 8, 593-604.
Ritov, I., & Baron, J. (1990). Reluctance to vaccinate:
omission bias and ambiguity. Journal of Behavioral Decision
Making, 3, 263-277.
Ritov, I., & Baron, J. (1999). Protected values and omission
bias. Organizational Behavior and Human Decision
Processes, 79, 79-94.
Slovic, P. (1998). Trust, emotion, sex, politics, and science:
Surveying the risk-assessment battlefield. In M. H. Bazerman, D.
M. Messck, A. E. Tenbrunsel, & K. A. Wade-Benzoni (Eds.)
Environment, ethics and behavior: The psychology of
environmental valuation and degradation, pp. 277-313. San
Francisco: New Lexington Press.
Tengs, T. O., Adams, M. E., Pliskin, J. S., Safran, D. G.,
Siegel, J. E., Weinstein, M. E., & Graham,
J. D. (1995). Five-hundred life-saving interventions and their
cost-effectiveness. Risk Analysis, 15, 360-390.
Ubel, P. A. (2000). Pricing Life: Why It's Time for
Health Care Rationing. Cambridge, MA: MIT Press.
Ubel, P. A., DeKay, M. L., Baron, J., & Asch, D. A. (1996).
Cost effectiveness analysis in a setting of budget constraints:
Is it equitable? New England Journal of Medicine, 334,
1174-1177.
Ubel, P. A., Baron, J., & Asch, D. A. (2001).
Preference for equity as a framing effect. Medical
Decision Making, 21, 180-189.
Viscusi, W. K. (2000). Corporate risk analysis: A reckless act?
Stanford Law Review, 52, 547-597.
Westfall, P. H., & Young, S. S. (1993). Resampling-based
multiple testing: Examples and methods for p-value adjustment.
New York: John Wiley & Sons, 1993.
Footnotes:
1This work was supported by a grant
from the Russell Sage Foundation. Author's address:
Department of Psychology, University of Pennsylvania, 3815
Walnut St., Philadelphia, PA 19104-6196
2Subjects were also more inclined to say
that the company should install the device than to say that the
agency should require it (.35 vs. .28, (t=2.82, p=.0058).
There is no hypothesis about this difference.
3Trust in B
was higher when the device is installed (the right two columns
of the table averaging .80) than when it is not installed (left
two columns .55, t=5.63, p=.0000), as if the thoroughness
mattered mainly when the agent did what most subjects thought
was the right thing, i.e., installing the device. But trust in
B was positive even when the device was not installed
(t94=9.94, p=0.0000).
4Company and agency did not differ.
5We also found a
triple interaction among knowledge, betterness, and benefit
[t=2.28, p = 0.0252]. The interaction between knowledge
and betterness was greater when benefit was higher [50 lives].
We find this difficult to interpret.
6Although men showed a smaller positive effect
of CBA on trust in Experiment 2 than did women, this result was
not found in Experiment 1, and it may thus be a fluke that
results from the small number of men in the sample, 29.
7Other data indicate that most subjects are
indeed typical for the U.S. population in income and education
(Babcock et al., 2003, whether they see themselves that way or
not.
File translated from
TEX
by
TTH,
version 3.40.
On 23 Nov 2003, 14:44.