The term hypnosis was coined in the 1840s by James Braid, a Scottish surgeon; it stems from the Greek hypnos ("sleep") and refers to a sleeplike state that nevertheless permits a wide range of behavioral responses to stimulation. The hypnotized individual appears to heed only the communications of the hypnotist. He seems to respond in an uncritical, automatic fashion, ignoring all aspects of the environment other than those made relevant by the hypnotist. Apparently with no will of his own, he sees, feels, smells, and tastes in accordance with the suggestions in apparent contradiction to the stimuli that impinge upon him. Even memory and awareness of self may be altered by suggestion, and the effects of the suggestions may be extended (posthypnotically) into subsequent waking activity.
The following descriptive account indicates what typically occurs in a hypnotic encounter. The person to be hypnotized (subject) is invited to relax in comfort and to fix his gaze on some object. The hypnotist continues to suggest, usually in a quiet, low voice, that relaxation will increase and that the subject's eyes will grow tired. Soon the eyes do show the normal signs of fatigue, and it is suggested that they will close. The subject will probably allow his eyes to close and then begin to show signs of profound relaxation such as limpness and regular breathing. The hypnotist now makes suggestions, typically in vivid, concrete terms; thus the subject may be told that his hand is so heavy that he cannot lift it but that he should try. The subject responds, often seeming quite puzzled by his inability to raise the arm. The hypnotist then tells him that it really does not matter, and he need not try any longer, that he is relaxing untroubled except for a mosquito buzzing around and landing on his forehead. The subject probably will grimace and may attempt to brush away or swat the imaginary insect. Relaxation is restored by the suggestion that the mosquito is flying away. It next may be suggested that as the insect departs the subject will totally forget what has happened this year, and last year, and the year before, back to (say) ten years ago. Shortly thereafter, the subject is invited to open his eyes, to walk about, and to engage in conversation. Asked the date, he may give some day a decade past;
133
134 Hypnosis
questioned about the recent news, he probably will describe political or social events of that time.
The session might be concluded by telling the subject that he is returning to the present time and that, on awakening at the count of ten, he will remember nothing of what has just happened until he is asked to relax and to recall everything. It is also suggested that, after the subject wakes, he will remove his wristwatch when he sees the hypnotist signal (e.g., by folding his arms). When he opens his eyes, the subject may act as if he suddenly finds himself in a strange place but seems to feel comfortable. Asked what has just occurred, he may say that he must have just dozed off; he cannot account for the period of hypnosis. If events which occurred during that time are described, he may deny that they did. Yet, when he sees the hypnotist fold his arms, he absent-mindedly takes off his watch. Asked why, he may rationalize by winding it and return it to his wrist. When the hypnotist later folds his arms, the subject again slips off his watch but may seem embarrassed by his own behaviour; he may begin to suspect that his actions have something to do with the hypnosis. Finally the subject may be asked to relax and, as the hypnotist counts to five, to recall everything that went on since he first was hypnotized. At the count the subject's expression usually will reveal a dawning awareness of the forgotten events. He may now describe his puzzling inability to lift his arm and his annoyance at the mosquito. He may also mention the awakening of memory as if part had been dissociated from awareness and then had suddenly become accessible and, further, his disappointment at knowing where he was and what he was doing.
In general, when a subject is hypnotized, he seems to accept as real the distortions of perception and memory suggested by the hypnotist, even though they surprise him. Activities such as grimacing at an invisible mosquito, quite unremarkable in themselves, strike the observer as strange because they imply the occurrence of perceptual experiences that are not usually brought about by simple assertion. Since, however, subjects characteristically report their experiences to others in much the same way as to the hypnotist, their behaviour cannot be explained as conscious playacting. In addition to responses explicitly suggested, subjects tend to show deep relaxation, regular breathing, passivity, and relative immunity to distractions.
HISTORY
Hypnotic techniques have been used since antiquity; healing practices by priests of ancient Egypt and Greece are striking examples. Trancelike behaviour attributed to "spirit possession" has played a role in Christianity, Judaism, and in many primitive religions. Miraculous powers ascribed to witches and the arts of faith healing throughout the ages are probably related to hypnosis.
The "discovery" of hypnosis in Europe is generally credited to Franz Anton Mesmer (1734-1815), an Austrian physician working in France at the time of the American Revolution. He found that some ailing people were benefitted by passing magnets over their bodies. Participants in his group seances sat around an open tub from which magnetized metal bars protruded; some would develop a "crisis" (a kind of convulsive fit), lapse into apparent sleep, and awaken cured or much improved. Mesmer later found that magnets were not crucial; it often seemed sufficient to touch the person or even to touch (or "magnetize") water before the sufferer drank it. Mesmer concluded that he was gifted with "animal magnetism," a kind of "fluid" that he could store and transfer to others to heal them. A follower of Mesmer, the nobleman Chastenet de Puysegur, "magnetized" a tree on his estate, at which his peasants would obtain relief from their ailments. By 1780 he had found that the "mesmeric crisis" was unnecessary and that he could influence a mesmerized person just by talking to him. He, in short, used hypnosis much as it is used today.
The notoriety that followed Mesmer's spectacular therapeutic claims led to the appointment in Paris of an investigating commission that included the American diplomat Benjamin Franklin and the French chemist AntoineLaurent Lavoisier. In 1784 it concluded that no magnetic "fluid" exists; striking recoveries from illness were not denied but attributed to "mere imagination." Thus discredited, hypnosis as a topic of objective investigation was neglected and tended to be linked with mysticism and quackery.
About 1840, physicians John Elliotson in London and James Esdaile in Calcutta made extensive use of mesmeric trance to carry out painless major surgery, including leg amputations. Elliotson endorsed belief in Mesmer's invisible "fluid" and held the metal nickel to be particularly useful in trance induction. The editor of the British medical journal Lancet surreptitiously exchanged nickel with lead; since the lead seemed to work just as well, he denounced such belief as "mesmeric humbug." Braid agreed that no magnetic "fluid" was involved but observed that people being treated with mesmerism seemed profoundly influenced. He introduced the term hypnotism to divorce the phenomenon from theories about animal magnetism and held that concentration on a single focus of attention (monoideism) was a major factor in the situation.
Hypnosis attracted widespread scientific interest in the 1880s as a result of a controversy in France. Ambroise-Auguste Liebeault, an obscure country physician at Nancy who used mesmeric techniques, drew the support of Hippolyte Bernheim, professor of medicine at Strasbourg. Independently they wrote that the phenomenon involved no physical forces and no physiological processes but were psychologically mediated responses to suggestions. In disagreement, Jean-Martin Charcot, professor of neurology at the Sorbonne in Paris, held that hypnosis occurs only in sufferers of hysteria, is therefore pathological, and does involve the influences of magnets and metals. (Charcot had become interested in the possible transfer of symptoms by magnets and in the effects of drugs at a distance.) History has shown that the effects of magnets and similar physical factors are really brought about by implicit psychological suggestions.
At about the same time, the Austrian physician Sigmund Freud visited France and was impressed by the therapeutic potential of hypnosis for neurotic disorders. On his return to Vienna he used hypnosis to help neurotics recall forgotten disturbing events. As he began to develop his system of psychoanalysis, theoretical considerations, as well as the difficulty he encountered in hypnotizing some patients, led Freud to discard hypnosis in favour of free association. Generally psychoanalysts have tended to view hypnosis as a somewhat masked intimate personal relationship.
Despite Freud's influential rejection of hypnosis, some use was made of the technique in treating combat neuroses during World Wars I and II. Pierre Janet in France and Morton Prince in the United States suggested that "dissociation of mental systems" is common both to the neurotic disorder called multiple personality and to the phenomenon of hypnosis. Prince showed that a hypnotized person seems to be able to carry on two or more independent streams of mental activity simultaneously.
Ivan Pavlov, the Russian physiologist, came to view sleep as reflecting widespread inhibitory processes in the brain and concluded that hypnosis is a similar inhibitory state in which there remain a few centres of neural excitation. His views enjoy wide acceptance among Soviet and eastern European workers who also tend to use prolonged periods of sleep in psychiatric therapy.
In America, experimental psychologist Clark Hull, applying controlled quantitative methods to the laboratory study of this complex and elusive phenomenon, concluded in 1933 that, as Bernheim had argued, hypnosis is best understood as a form of hypersuggestibility. Important basic research has continued in Hull's tradition with normal volunteer subjects. A combined clinical-experimental approach, inspired by Milton Erickson's pioneering work in the 1940s, has been effective as a research strategy and has led to novel therapeutic applications which have helped spark renewed widespread interest in hypnosis.
135 Hypnosis
Scientific journals devoted exclusively to hypnosis are published in England, Japan, South America, the U.S., and Sweden. National societies in many countries hold annual scientific meetings, and international congresses on hypnosis have been held in France (1965), Japan (1967), Germany (1970), and Sweden (1973).
MODERN THEORIES
Despite active empirical study of hypnotic phenomena, there is no single generally accepted explanatory theory. Some theorists influenced by Pavlov think of hypnosis as a state of altered consciousness or partial sleep in which a person tends to respond to suggestions automatically and uncritically. While this view does not ignore increased suggestibility, it still holds that a subject not at the moment responding to a suggestion may nevertheless be in a trance state. There may be neurophysiological components of such a state. Such a position would be consistent with the notion, not generally accepted, that some animals can be hypnotized, as when a chick, suddenly placed on its back, tends to remain immobile in that position (see DORMANCY).
Other theorists stress the social or interpersonal interactions that hypnotic behaviour involves. They emphasize how an actor willingly and wittingly permits a director to guide him into living a part; how a patient may be relieved of a headache if given a pill that is actually pharmacologically inert (a placebo); how an uncommitted person becomes an enthusiastic supporter of crowd feeling at a demonstration; how a spectator flinches and jabs along with his favourite fighter; and how a student changes his views to those of an admired teacher. Hypnosis is held to consist of nothing more than events like these, there being no need to assume additional special states such as the inhibition of parts of the brain. Hypnotic events are results of interpersonal influences in which various abilities, skills, and response propensities are brought into play.
Evidence can be found to support both major theoretical approaches. Neural changes indeed do occur in hypnosis, but a unique physiological basis for the phenomenon remains to be established. Perhaps this reflects incomplete understanding of physiological alterations that may produce psychological change. Social-interaction theorists find it difficult to explain why posthypnotic suggestions are carried out even when the hypnotist neither knows nor apparently cares about the subject's behaviour. While most current investigators tend to work within one or the other explanatory framework, most feel free to use propositions from both if they seem consistent with experimental or clinical observations.
INDUCTION OF HYPNOSIS
Techniques to induce hypnosis share common features. Responsiveness is maximized when the subject seems to believe that he can be hypnotized, that the hypnotist is competent and trustworthy, and that the undertaking is safe, appropriate, and congruent with his wishes. Therefore induction is generally preceded by the establishment of suitable rapport between subject and hypnotist. After this the hypnotist proceeds to try to focus attention on the procedure proper.
Ordinary inductions begin with simple suggestions that will almost inevitably be accepted by all subjects. At this stage neither subject nor hypnotist can readily tell whether the subject's behaviour constitutes a hypnotic response or mere cooperation. Then, gradually, suggestions are given that demand increasing distortion of perception or memory. In the eye-closure method described above, for example, the suggestions of visual fatigue are consistent with and take advantage of normal strain during fixation and thus serve to heighten expectations of positive response. It is difficult for hypnotist, subject, or outside observer to be sure whether eye closure indicates hypnosis or mere voluntary compliance. But the hypnotist gradually moves on to suggest that it will be difficult or impossible to open the now-shut eyes. Although not all subjects respond positively, those who do seem to have gone beyond the point of simple compliance. By linking any successful responses with ensuing suggestions, the hypnotist often can elicit increasingly marked distortions of perception, belief, memory, and attitude. The success or failure of any suggestion is considerably influenced by how well the hypnotist observes and uses the subject's natural talents.
While induction is usually carried out in a quiet, dimly lit room, it may be done in normal illumination. The subject may be asked to attend to any of a wide variety of stimuli--his own hand, his breathing, an imaginary visual image, or a tone. He need not be seated and relaxed; indeed, in some methods the subject is asked to tense his muscles. Even carefully selected distractions can be used to facilitate progress.
Induction of hypnosis may take considerable time but sometimes requires only a few seconds. Hypnotists in theatres and night clubs capitalize on developing appropriate expectations and selecting individuals ready and willing to enter, deep hypnosis. Much of the effort in clinical settings is directed toward establishing appropriate attitudes in the subject. The advertising and publicity given the stage hypnotist before he faces the audience likewise facilitate response; with such preparation, he sometimes can induce hypnosis all but instantaneously, merely by shaking a particularly susceptible subject's hand or by saying in a commanding voice, "Sleep!" Given suitable preparation, tape-recorded induction procedures may be as effective as an experienced hypnotist.
With suitable subjects hypnosis also can be induced by a series of suggestions without any reference to sleep or eye closure. Some waking individuals go directly into the same state produced by telling a deeply hypnotized subject that he will open his eyes while in the trance.
In general, hypnosis cannot be induced against an individual's will. Occasionally experiments have been reported in which individuals were asked to resist but nonetheless were hypnotized. In all such examples the hypnotist solicited the subject's cooperation in an experiment; only then did he ask for resistance. Assuming the subject is capable of hypnosis, his response seems to depend on whether he wishes to help in solving the experimental problem or whether he wants to follow the specific instruction to resist. It is unwarranted to assume that under these circumstances the subject truly does not wish to enter hypnosis; it has not been convincingly shown that hypnosis can be induced in someone independently motivated to resist. This does not mean, however, that a willing person cannot be hypnotized without his formal consent. It is unusual, but in some therapeutic or religious contexts, for example, people have been observed to exhibit trancelike or hypnotic behaviour without evidence of intention on their part or even on the part of a hypnotist.
Hypnotic suggestions. A peculiar quality of speech seems helpful in making hypnotic suggestions. Most people can identify the voice quality, traditionally described as monotonous and repetitious but probably more accurately as intense, insistent, and simple. Suggestions seem most effective when the hypnotist paints a vivid word picture of concrete images that are easily imagined.
Suggestions also are best given in indicative rather than imperative form. Instead of saying, "Lift your hand," for example, the hypnotist encourages a passive attitude in which the subject neither strives to help nor to hinder the arm and says, "It is becoming light ... the fingers are beginning to rise ... they feel like balloons as they float into the air. ..."
As the subject begins to respond, the hypnotist often behaves as if he shares the subject's unusual experiences. When, for example, the person seems to be hallucinating a familiar friend in response to suggestion, the hypnotist may ask to be introduced. He will begin to talk to the subject's hallucination as if he too were seeing the imaginary person.
The popular impression of the hypnotist as authoritarian and dominating fits the behaviour of many stage hypnotists and of psychiatrists using hypnosis in the last century. Just as the authoritarian bedside manner of medical practitioners is no longer the norm, however, so has the
136 Hypnosis
approach of the medical hypnotist changed with the times. Under most circumstances, therapeutic hypnosis is now carried out in an atmosphere of cooperation, the hypnotist assuming the role of a teacher who can help his student achieve a mutually sought goal.
Technical aids. A wide variety of devices has been employed to facilitate fixation. A rotating picture of a spiral has been popular, its movement tending to focus attention on the centre. Arrangements of mirrors and fixation points also have been used, just as the subject may focus attention on his own breath sounds. Particular theoretical interest has been shown in the use of a flashing light, especially when adjusted to the subject's own electrical brain rhythms (typically nine or ten pulses per second).
Drugs also have been used, especially sedatives (e.g., barbiturates) for relaxation prior to hypnotic induction. (Paradoxically, injections of such stimulants as amphetamines also have been reported to help.) Any procedure that produces momentary clouding of consciousness can be used to activate responses to suggestions. Hypnotic efforts are enhanced when a person is drowsy or about to fall asleep (with or without drugs). Similarly, dulled awareness readily can be achieved by pressure on blood vessels in the neck to deprive the brain of oxygen. This potentially injurious technique most often is employed by medically untrained hypnotists. There also is some indication that people under sensory deprivation (conditions of silence, darkness, and isolation) become unusually suggestible.
These procedures appear effective primarily in heightening expectations; it has never been shown that persons who are not susceptible to ordinary induction procedures abruptly become hypnotizable with these aids.
HYPNOTIC PHENOMENA
Appropriate suggestions can induce a remarkably wide range of psychological responses among deeply hypnotized persons.
Ideomotor responses. When one vividly imagines moving his body, he has a marked tendency to do what he is thinking. If the responsive subject stands with his back to the hypnotist, for example, and it is suggested that he is falling backward farther and farther, as he concentrates he will begin gradually to sway in that direction. Similarly it may be suggested that his hand will grow lighter and float upward or that it will become heavy and be pulled down. Waking individuals also respond to suggestions of movement, and there is some question whether hypnotic induction increases the probability of such behaviour. Since the tendency of subjects to respond to suggested movement is related to their general suggestibility, such ideomotor phenomena are widely considered to be a kind of hypnotic response.
Challenge suggestions. Challenge suggestions are those in which the subject is told he is unable to implement his own will; for example, "Your eyelids are shutting tight ... tighter ... tighter. You cannot open them even if you try.... Try to open them.... You cannot.... They are stuck together." Similarly, a hypnotized subject may be informed that his eyelids will force themselves open despite his effort to keep them shut. Challenge suggestions are of theoretical interest in that they seem to prevent voluntary action, striking observer and subject as dramatic demonstrations of external control over the individual. Such experiments have little therapeutic application; they also can be carried out with some people without formal hypnotic induction procedure, although response to challenge tends to be augmented during trance states. Response among waking individuals can serve as a test of hypnotic susceptibility; generally, those who respond very positively to challenge subsequently are found to be deeply hypnotizable. Challenge items emphasize the compelling character of hypnotic suggestion.
It has been observed that challenge suggestions may impose a logical "double bind"; e.g., that the instruction to try actually means to attempt and fail to open one's eyes. Some theorists suggest that it is not possible to comply with the instruction to try to open one's eyes and at the same time to cooperate with the generic instruction to be hypnotized. Whatever the validity of this theoretical formulation, many subjects say they feel genuinely unable to overcome such a challenge.
Perceptual distortions. With appropriate suggestion, the hypnotic subject may perceive stimuli not actually present or fail to perceive stimuli that are present. In response, for example, to the suggestion that an absent person is present, the subject may report that he sees, hears, and feels the hallucinated person and even spontaneously carry on a conversation with the hallucinated image.
Other perceptual distortions, such as feeling warm or cold or having a sweet or acid taste, may readily be suggested. It is typically easier to induce illusory experience--for example, that a lemon is a peach of which one can enjoy the delicate flavour--than to produce a positive hallucination in the absence of external objects. The most difficult to elicit are negative hallucinations in which the subject seems unable to perceive objects actually present.
Hypnotic analgesia and anesthesia may involve both the reduction of fear, relatively easily achieved by hypnosis, and the more difficult negative hallucination of pain. Since anticipation of pain tends to heighten discomfort substantially in the dentist's chair, some dentists report that more than 90 percent of their patients show a greatly increased pain threshold and a marked reduction in the need for local anesthesia even under light hypnosis. Such results largely stem from the effect of hypnosis on the reduction of fear; on the other hand, major surgical operations can be performed without anesthetic drugs but require deep hypnosis. This seems feasible with a much smaller number of individuals, and such anesthesia is likely to involve a negative hallucination of the pain experience.
Negative hallucination also seems to be a major part of hypnotic rapport. Once hypnosis is induced, subjects typically ignore all stimuli but the hypnotist. This appears to be a response to the suggestion to ignore the environment (e.g., "You will pay attention only to my voice."), a kind of negative hallucination for everything outside the hypnotic context. Nevertheless, once hypnotic rapport has been established, it can readily be transferred by suggestion from the hypnotist to someone else.
Alterations of memory. Among the most dramatic experiences of the hypnotized individual are distortions of recall. If it is suggested that fictitious events really have occurred, the subject may not only seem to remember them, he may also elaborate on them. Suggestions may be given to forget what happened yesterday or one's own name. Told to forget the number 6, for example, a subject will count his fingers as ... 5, 7, 8 . . ., ending with what he seems to perceive as an 11th finger. Encouraged to explore this peculiarity, he may note that he can count five fingers twice with no difficulty and correctly conclude that there must be a problem with his ability to count between five and ten. Yet this inference does not necessarily help him to recall the missing number.
A special case of memory distortion is hypnotic age regression; an adult, for example, appears to relive events that occurred when he was a child--his speech, writing, and general motor behaviour becoming childlike. He appears to recall events and skills long since lost or forgotten, such as playing a musical instrument or speaking a foreign language learned in childhood. Some investigators have taken the phenomenon of age regression as evidence for total storage of all sensory impressions, but carefully controlled studies generally have failed to find support for this assumption. When verifiable details of memory are checked, there seems to be little recall of factual information beyond what was available in the adult waking state.
Hypnotic age regression does seem to make the subject less concerned about the accuracy of his memory, and he fills in memory gaps with vivid imagination. This in turn may promote recall of repressed, emotionally charged actual experiences; however, even then it is often difficult to distinguish fact from fiction. The individual may be both convinced and convincing despite a tendency to elaborate, embroider, and distort what actually occurred.
137 Hypnosis
Hypnotic age regression has been advocated and used in legal cases. Great care should be taken in evaluating the accuracy of testimony even if the witness seems to be totally convinced of the honesty of his report. Hypnosis is no guarantee against falsification.
It remains controversial whether hypnotic suggestions can improve memory effectively. The effect, if any, is small for the kinds of information ordinarily employed in laboratory studies of learning and forgetting. The popular opinion that hypnosis facilitates recollection has not been supported by adequately controlled subsequent research. The common belief of the student who has neglected his studies that through hypnosis he may recall enough to pass his examinations, sadly, lacks reliable foundation.
Posthypnotic amnesia. Many subjects seem unable to recall what happened while they were in deep hypnosis. It is unclear whether this posthypnotic amnesia is a spontaneous consequence of deep hypnosis or whether it results entirely from suggestion. While suggestions made during hypnosis do have substantial effects on what the subject subsequently recalls, it remains to be shown that they account for all posthypnotic remembering or forgetting. Posthypnotic amnesia may be successfully removed by appropriate hypnotic suggestions.
Other kinds of hypnotic suggestions. Delusions. Appropriate hypnotic suggestions also can prompt the subject to embrace false beliefs (delusions). Told that he is a famous actor on his way to a television interview, the hypnotized person will show through his posture, mannerisms, attitudes, and speech clear alterations that are consistent with the delusion. Deluded behaviour also may be elicited through age progressions, in which it is suggested to a young adult, for example, that he is now an old man. The ease with which subjects respond to suggestions of age progression indicates that age regression, including regression to previous "incarnations," may be equally delusional.
Time distortion. Suggestions may be given that the passing of time will speed up or slow down. In the latter case, for example, a hypnotized subject may seem to experience a full-length motion-picture film in only a few seconds. It is quite unlikely, however, that such hypnotic time distortion can in reality accelerate the learning of new information.
Attitude change. Of special therapeutic potential is the effect of hypnotically suggesting altered attitudes. It may be suggested to someone who feels unattractive, for instance, that he will find that people like him and are drawn to his company. When used judiciously, suggestions such as these may result in enduring therapeutic changes by modifying the person's behaviour toward others. To the degree that his new optimism leads to friendlier, more confident approaches to people, their typically reciprocal responses will reinforce the changes initiated by hypnotic suggestion.
Physiological alterations. A broad variety of bodily changes have been produced by suggestion in hypnotized individuals. These usually are elicited indirectly by mentioning appropriate circumstances; for example, viral cold sores (herpes) have been induced, not by directly suggesting their appearance but rather by suggesting emotional distress of the sort that previously was associated with their eruption. Similarly, suggestions that they feel cold lead some subjects to show such bodily signs as shivering and circulatory alterations. Suggested sudden pain, discomfort, or stress can change the electrical resistance of the subject's skin and alter his respiration and heart rate. On the other hand, successful suggestions of diminished pain do not seem to abolish such bodily responses to the stress.
There is controversy about the hypnotic induction of blisters. Told that a cool coin touching him is red hot, a subject shows intense discomfort; sometimes there may be redness and blistering skin. Generally not reproducible under controlled laboratory conditions with normal volunteer subjects, psychologically induced blisters seem most likely to appear only in those prone to convert emotional disturbances into symptoms of skin disease.
Although some surgeons and many dentists report hypnotic control of bleeding after such procedures as tooth extraction, this remains to be verified by controlled experiment.
Posthypnotic suggestion. A deeply hypnotized individual can be induced to carry out an action in response to a specific cue some time after trance termination. With adequate amnesia, he will not be aware of the source of his impulse to act and may rationalize his behaviour. Even with awareness, he may still feel compelled to carry out the action and, if he attempts to resist doing so, evidence of conflict can usually be observed.
Posthypnotic suggestion, however, is not a particularly powerful means of controlling behaviour. Simple requests to a cooperative individual are responded to more consistently and over longer periods than posthypnotic suggestions. A group of subjects in deep hypnosis, for example, given postcards and instructed to mail one every day, sent fewer cards than others merely asked to carry out this action. This holds for trivial tasks, easily carried out, but the situation is reversed when the suggestion concerns behaviours the individual has difficulty in controlling himself.
Thus, posthypnotic suggestions have been quite effective in the treatment of habits such as smoking. In these instances, the posthypnotic suggestion is congruent with the individual's desires and reinforces them. Efforts to use posthypnotic suggestion as a means to force an individual to behave in a manner undesirable to him are usually doomed to failure, though such suggestions may occasionally lead to troublesome mental conflict.
In contrast to a simple request, posthypnotic responses are carried out not simply to please the hypnotist, but rather they may persist even in private when the hypnotist apparently could not know or care about the execution of the action.
All phenomena that can be elicited during hypnosis can, in suitable subjects, be elicited posthypnotically. This raises serious theoretical issues and has led some theorists to argue that the posthypnotic cue reinstates hypnosis.
LIMITATIONS AND POTENTIALITIES OF HYPNOSIS
The objectively observable phenomena of hypnosis are not so different from those of voluntary waking cooperation as once was supposed. It has been shown that during a lecture a student asked by his teacher to take off his shoe, to exchange neckties with a neighbour, or engage in other slightly embarrassing, ludicrous actions will do so. Had hypnosis first been induced, observers might have wrongly concluded that the subject was in the "power" of the hypnotist.
When unhypnotizable subjects are asked to simulate hypnosis, their performance can deceive experienced hypnotists. Simulating subjects convincingly perform extraordinary feats of strength and memory; for example, tolerating a needle through the arm without flinching. Such feats have mistakenly been taken as proof that hypnosis confers abilities that transcend those of waking activity.
Investigators once were inclined to conclude that deeply hypnotized subjects can be compelled against their "will" to carry out self-damaging and antisocial behaviour. They cited independent studies demonstrating that such individuals will attempt to pick up a poisonous snake, to pick up with their bare fingers a coin dissolving in a beaker of fuming nitric acid, and to throw the acid at a research assistant. Asked in the waking state whether they would obey such suggestions, the same subjects were quick to deny the possibility. In subsequent work, however, deeply hypnotized people were mingled with simulating subjects without the experimenter's knowledge, which ensured that he treated all subjects in the same persuasive way. Instructed to carry out these perilous, undesirable acts, five out of six hypnotized subjects did so, but all of six simulators did likewise. The experiment demonstrates that different answers emerge when waking subjects are asked whether they will carry out an action and when they are instructed to do so in a way that
138 Hypnosis
clearly communicates expectation of compliance. Under the latter circumstances waking subjects correctly seem to surmise that safety precautions have been taken; indeed, no responsible investigator permits subjects or assistants to be hurt. The further implication is that the genuine hypnotic subjects also may have surmised that the situation was safe; it thus remains undemonstrated that they were under the hypnotist's "power."
This experiment is typical of a number of controlled studies that call many earlier extravagant claims about hypnosis into serious question. It now seems quite unlikely that the hypnotized person can transcend his waking potentials in physical strength, perceptiveness, learning ability, and productivity. Similarly, it seems most improbable that hypnotized people can be compelled to do what they would be most unwilling to do in the waking state. But hypnosis may be used, as various other methods may also be used, to induce a person to alter his usual behaviour.
The inability of the hypnotized subject to transcend his waking potential does not call into question the reality of hypnosis. When a hypnotized person reports a hallucination, all the evidence indicates that it is real to him. The significant aspects of hypnosis are found in the quality or characteristics of the subject's induced experiences. The statements of people after trance indicate that hypnotic experiences are qualitatively distinct from those reported by simulators. Genuinely hypnotized subjects, for example, tolerate the discrepancy of actually seeing a person and of simultaneously hallucinating that person at another location without being especially cued; this does not hold for the simulator. Hypnotized people tend to carry out suggestions during or after trance whether the hypnotist is present or not; simulators cease to respond when they are quite sure they have no audience.
Altogether then, hypnosis should not be considered as a technique for achieving supernormal performance or control. Rather it is a collaborative enterprise in which the inner experience of the subject can be dramatically altered.
Hypnotic responsiveness. Some suggestions, such as those of eye closure and feelings of heaviness, warmth, and relaxation, are effective with most individuals. Other suggestions, including those of analgesia to a pinprick or difficulty in opening one's eyes when challenged, elicit positive responses from a lesser number. Hallucinations, general posthypnotic amnesia, and other memory distortions are achieved only in approximately one-quarter of the population; negative visual hallucinations, profound surgical anesthesia, and response to bizarre posthypnotic suggestions are feasible with only a few people. On this evidence, items of suggestion can be graded roughly in terms of difficulty. Occasionally a subject may respond to a generally difficult item and not to one that is rated easy, but this is not the usually observed pattern.
Such data have led to the development of a number of standardized scales for assessing hypnotic susceptibility. Designed for research with normal subjects, they avoid highly personal or emotionally upsetting items. TheStanford Hypnotic Susceptibility Scales are widely used. Some, consisting of easier items, are used for preliminary screening. Others contain more difficult items, and some are designed to reveal the particular kinds of suggestion to which the subject best responds. Variations of the Stanford scales include the Children's Hypnotic Susceptibility Scale and the Harvard Group Scale, the latter also employing tape-recorded procedure.
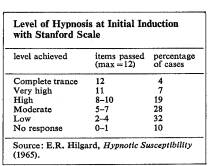
Scales of this sort are fairly reliable in that most subjects' responses are reasonably stable from one time to another and from one form of the scale to another. (If a person chooses to resist, the hypnotic procedure, however, he will score low even though he may be quite capable of responding. Susceptibility scales, like intelligence tests, can be misleading unless the individual tries his best.) The Table summarizes typical variations in depth of hypnosis induced among normal college students with a graded series of items from the Stanford scales.
Any individual's overt responses to a standardized scale may be objectively scored and evaluated against such a
table of norms. The investigator also may ask the individual how strongly he felt affected by the procedure. Results from objective scoring and from the person's subjective report tend to yield similar estimates of depth of hypnosis, but concordance is far from perfect. One subject may give marked overt responses but later say that he merely was trying to be helpful; another more lethargic person may not emphatically respond but subsequently may report profound awareness of hypnotic change. Such verbal reports are of particular interest in clinical, therapeutic settings.
Some subjects manifest very deep hypnosis in responding to even the most difficult items yet later say their experiences differed little from the fantasy of ordinary daydreaming. Others who fail to respond to all of the more difficult suggestions nonetheless seem deeply affected by the discovery that they have responded at all. They may say that having their eyes grow heavy was vastly different from, and more impressive than, any other experience they can recall. In therapeutic contexts this latter evidence of hypnotic depth often seems closely related to the individual's attitude toward his therapist. Probable therapeutic response, however, has not been shown to be adequately predictable from any of these criteria of depth of hypnosis. Sufferers have been deeply hypnotized in terms of all such criteria and have failed to be relieved of their psychiatric symptoms; others who seem barely affected during hypnotic efforts nevertheless show substantial improvement under hypnotic treatment.
Effect of repeated hypnosis. Initial anxiety or conflict about entering hypnosis generally interferes with an individual's responsiveness. Subsequent improvement of rapport with the hypnotist and growing familiarity with the procedure help many subjects to produce more profound experiences, but each soon reaches a particular plateau at which the kind of phenomena elicited seems to stabilize. Practice beyond this point, however, does tend to increase the speed of response, which may account for the widely held belief that depth of hypnosis continues to improve with practice.
The posthypnotic suggestion often is given that a subject in future will immediately enter a trance on a specified cue. The ease and rapidity with which this can occur in a trained subject should not be taken to mean that he is becoming more susceptible, nor that he cannot resist if he truly wishes to do so.
Undue dependence on the hypnotist does not ordinarily occur in experimental work but has been reported for some therapeutic relationships. Such a response may complicate all forms of therapy but is most likely to occur with lay hypnotists and other individuals who ineptly attempt psychotherapeutic interventions without appropriate training and experience.
Hypnotizability. The stability of one's hypnotic responsiveness seems as great as that of other abilities such as mechanical or verbal skills, and much research has been devoted to the search for personal attributes related to hypnotizability. Early investigators assumed that women enter hypnosis more readily than men, but this has not been borne out in most studies; similarly, hypnotizability is not especially related to intelligence nor to education. There does appear to be a significant relationship with age, ability to respond reaching a peak before puberty, stabilizing in the early adult years, and declining in very old age. Traits popularly characterized
139 Hypnosis
as evidence of gullibility are not related to hypnotizability. There is some indication that a history of parentally approved daydreaming, fantasizing, and imaginative play during childhood is associated with increased ability to respond. The extent to which an individual spontaneously becomes absorbed in a play to the point of feeling the emotions portrayed also has some predictive value. There is evidence that hypnotizability is greater among individuals who seem generally well adjusted. Among those with psychiatric disorders, hysterics respond better than others. Most individuals with obsessive-compulsive or schizophrenic symptoms are unresponsive, but even with these difficulties some can enter deep hypnosis.
EVALUATION OF THE APPLICATIONS OF HYPNOSIS
By the 1970s hypnosis had been officially endorsed as a therapeutic method by medical, psychiatric, dental, and psychological associations throughout the world.
Because of the availability of safe and effective anesthetic drugs, hypnosis is used in major surgery only rarely. On the other hand, it has been found most useful in preparing people for anesthesia, enhancing the drug response, and reducing the required dosage. In childbirth it is particularly helpful, since it is effective in alleviating the mother's discomfort while avoiding drug-induced impairment of the child's physiological function. The technique also has been helpful in painful, relatively minor procedures such as changing dressings over severe burns. Hypnosis is highly regarded in the management of otherwise intractable pain, including that of terminal cancer. It is valuable in reducing the widespread fear of dental procedures; the very people whom dentists find most difficult to treat frequently respond best to suggestions. It has also proven useful in such aspects of dentistry as suppressing undesirable gagging reflexes and in helping people adapt to new dentures.
In the area of psychosomatic medicine hypnosis has been used in a variety of ways. Patients have been trained to relax and to carry out, in the absence of the hypnotist, exercises that have had salutary effects on some forms of high blood pressure, headaches, and functional disorders. Specific suggestions have also been used in some of these contexts but tend to have limited applicability compared with more general procedures designed to reduce the patient's tension. Many fascinating isolated case reports of dramatic therapeutic changes induced by hypnosis, especially in dermatology, are in the literature, but overall effectiveness in dermatology has not yet been adequately evaluated. In many instances, the appropriate treatment for psychosomatic difficulties is psychotherapy, in which hypnosis may or may not be included.
The use of hypnosis in psychotherapy. In psychotherapy, hypnosis has been used in a variety of ways. Specific suggestions to relieve troublesome symptoms have limited utility. Those symptoms that may be suppressed with confidence and safety are the ones least likely to be central problems to the patient, and considerable care should be taken in evaluating the nature of the problem before such treatment is undertaken. The use of hypnotic suggestions to change psychological attitudes has been mentioned. The technique of revivifying traumatic events, leading to a cathartic emotional release, was originally employed by Freud and continues to be a useful treatment in relieving neuroses with traumatic onset (see PSYCHONEUROSES), such as those that develop in combat, among individuals with relatively stable prior adjustments. There are a variety of other, more specialized ways in which hypnosis has been employed to help patients understand their own reactions and to become aware of their own feelings. Hypnosis itself is never the treatment, however; rather, it is a technique used in the context of an overall treatment approach. It has been used in modern behaviour therapy, for example, as well as in psychoanalytically oriented approaches. In countries where the Pavlovian school is particularly important, there has been a tendency to employ prolonged hypnotically induced sleep as a way of bringing about curative rest.
General comments about the use of hypnosis in treatment. The induction of hypnosis requires little training. Though the technique and skill of the hypnotist are not totally irrelevant, the personality and motivation of the subject and his interaction with the situation are of paramount importance. Nevertheless, there is an erroneous though widely held belief that individuals capable of inducing hypnosis have some special power or skill that makes them equipped to treat. Congruent with this belief is the view that there is a science of hypnosis.
While an appropriate topic of scientific inquiry, hypnosis is not a science in its own right. On the contrary, it is the task of psychological science to discover how hypnosis can be accounted for by its general laws While little skill is required to induce hypnosis, considerable training is needed to evaluate whether it is the appropriate treatment technique and, if so, how it should properly be employed. When used in the treatment context, hypnosis should never be employed by individuals who do not have the competence and skill to treat such problems without the use of hypnosis. For this reason hypnosis "schools" or "institutes" cannot provide the needed training for individuals lacking the more general scientific and technical qualifications of the healing professions. In most major cities individuals advertise in the classified sections of telephone books as professional hypnotists, offering to treat a wide range of medical and psychological problems. Since the ethical codes of the professions would prevent any physician, psychologist, or dentist from advertising in such a fashion, individuals who consult someone who holds himself out to be a hypnotist should be aware that such a person is extremely unlikely to have the necessary training or skill to treat medical or psychological problems. Improperly used, hypnosis may add to the patient's psychiatric or medical difficulties. Thus, a sufferer of an undiscovered brain tumor may sacrifice his life in the hands of a practitioner who successfully relieves his headache by hypnotic suggestion, thereby delaying needed surgery. Broad diagnostic training and therapeutic skill are indispensable in avoiding the inappropriate and potentially dangerous use of hypnosis.
Interrogation and discovery of truth. Hypnosis has not been found reliable in obtaining truth from a reluctant witness. Even if it were possible to induce hypnosis against one's will, it is well documented that the hypnotized individual still can willfully lie. It is of even greater concern that cooperative hypnotized subjects remember distorted versions of actual events and are themselves deceived. When recalled in hypnosis, such false memories are accompanied by strong subjective conviction and outward signs of conviction that are most compelling to almost any observer. Caution and independent verification are essential in such circumstances.
Augmenting performance. Hypnosis used in attempts to increase athletic prowess usually yields equivocal results. Psychological factors clearly affect performance, and under some circumstances one might expect that hypnosis could be effective; nevertheless, it is seriously questioned whether it ought to be employed in competitive athletics. The widespread belief that hypnosis facilitates total recall is an irresistible idea, especially to students about to be examined. As noted earlier, objective evidence unfortunately fails to support this belief; hypnosis has not been particularly effective as an adjunct to memory or recall. Equal or better performance can be obtained by motivating individuals in other ways.
Antisocial uses of hypnosis. Despite many fictional stories about the use of hypnosis to persuade victims to help in criminal acts, no authenticated instance has come to light where hypnosis was successfully employed to force a person to act criminally to the advantage of the hypnotist, in the absence of an intense personal (but nonhyhypnotic) relationship with the hypnotist, or a pre-existing willingness to behave criminally. The dangers of anti. social use have been greatly exaggerated.
Future directions in hypnosis. The story of hypnosis illustrates errors not infrequent in the history of science in general. As Mesmer was. other theorists are over.
140 Hypnosis
ready to extend a concept beyond the limits of its applicability. Critics, with due regard for evidence, expose the error, but, overdoing skepticism, often fail to discern the real grain of truth in the original material. In the long run, progress is achieved by dint of a succession of nearer approximations. At any time, the way new data are handled depends markedly on the state of science at that time.
Full understanding of hypnosis depends on the state of psychological and psychiatric science. There can be no separate science of hypnosis. More particularly, when there are improved techniques of describing and quantifying mental states and subjective experiences, and greater knowledge of the physiology underlying attention and reality-testing, then a more adequate explanatory account of hypnosis will become possible. However, progress in hypnotic research will not await those achievements, but rather will contribute to them, just as hypnotic studies have already contributed insights about unconscious mental processes, about psychological influences in somatic illnesses, and about the powerful effects of expectations on behaviour.
BIBLIOGRAPHY. A classic of historical interest in its emphasis on the psychological character of hypnosis is H. BERNHEIM, Hypnosis and Suggestion in Psychotherapy (Eng. trans.1888, reprinted 1964). Also of historical interest is C.L. HULL, Hypnotism and Suggestibility: An Experimental Approach (1933), the first major systematic effort to study hypnosis in the psychological laboratory. On techniques, a comprehensive treatment of induction and therapeutic application, supported by detailed illustrations, is L.R. WOLBERO, Medical Hypnosis, vol. 1, The Principles of Hypnotherapy, vol. 2, The Practice of Hypnotherapy (1948). A current account of experimental studies of hypnosis, including a substantial amount of original research, is E.R. HILGARD, Hypnotic Susceptibility (1965). M.T.ORNE, "Hypnosis, Motivation and the Ecological Validity of the Psychological Experiment," a paper in the, Nebraska Symposium on Motivation (1970), summarizes empirical work, documenting both the limitations of hypnosis and some of its unique attributes. No single volume adequately covers theorizing about hypnosis. M.M. GILL and M. BRENMAN, Hypnosis and Related States (1959), presents a psychoanalytically oriented theory of hypnosis; TX BARBER, Hypnosis: A Scientific Approach (1969), a skeptical view. Contributions of other theorists, especially those of White, Kubie, Sarbin, and Erickson are included in the collection of basic readings: R.E. SHOR and M.T. ORNE (eds.), The Nature of Hypnosis (1965).
(M.T.O./A.G.H.)