Pre-publication copy of the paper eventually published as Shapiro, B.S., Dinges, D.F., Orne, E.C., Bauer, N., Reilly, L.B., Whitehouse, W.G., Ohene-Frempong, K., & Orne, M.T. Home management of sickle cell-related pain in chidren and adolescents: Natural history and impact on school attendance. Pain, 1995, 61, 139-144
Barbara S. Shapiro, M.D.1, David F. Dinges, Ph.D. 2 , Emily Carota Orne 2, Nancy Bauer, M.S.S. 2, Linnette B. Reilly, R.N., B.S.N., Wayne G. Whitehouse, Ph.D. 2, Kwaku Ohene-Frempong, M.D. 3, Martin T. Orne, M.D., Ph.D. 2
1. Division of General Pediatrics, Children's Hospital of Philadelphia, and University of Pennsylvania School of Medicine.
2 Unit for Experimental Psychiatry, Institute of Pennsylvania Hospital, and University of Pennsylvania School of Medicine.
3 Division of Hematology, Children's Hospital of Philadelphia, and University of Pennsylvania School of Medicine.
Address correspondence and requests for reprints to Barbara Shapiro, M.D., Children's Hospital of Philadelphia, Division of General Pediatrics, 34th Street and Civic Center Blvd., Philadelphia, PA 19104.
We acknowledge the help of Michele Carlin, Geoffrey Ott, and Kelly Gillen in analyzing the data.
Supported in part by NIH grant MH44193, and in part by grants from Hasbro Children's Foundation, van Ameringen Foundation, Stratford Foundation, and the Institute for Experimental Psychiatry Research Foundation.
1 Home Management of Sickle-Cell Pain
ABSTRACT
Some children and adolescents with sickle cell disease experience frequent painful episodes. To gain information about the natural history of the pain and its impact on sleep and school attendance, we developed a home-based diary system. Eighteen children and adolescents completed 4,756 diary days, with an average compliance of 75%. Pain was reported on 30% of days, and was managed at home nine-tenths of the time. Girls reported more days with pain than did boys, and age was positively correlated with the length of the painful episodes. The pain affected school attendance and sleep. Patients were absent from school on 21% of 3,186 school days, with half of the absenteeisms on days with reported pain. Of the pain associated absenteeisms, two thirds occurred when pain was managed at home, and one third when patients were hospitalized. The average consecutive number of school days missed was 2.7. These findings have implications for developmentally critical activities.
Key Words: pain, sickle cell disease, crisis pain, painful episode, chronic illness, sleep, school.
2 Home Management of Sickle Cell Pain
INTRODUCTION
Vaso-occlusive pain is the most common problem encountered by patients with sickle cell disease (SCD)(Tetrault et al. 1974). The pain, which is intermittent, often severe, and unpredictable, can start as early as 6 to 9 months of age, and continues throughout adulthood (Serjeant 1985). The pain frequency and severity varies greatly among and within individuals (Serjeant 1985; Vichinsky et al. 1982), with a minority of patients experiencing frequent and severe painful episodes (Vichinsky et al. 1982). Many studies of the natural history and treatment of SCD related pain utilize emergency department and inpatient admissions as indicators of pain severity and frequency (Platt et al. 1991). However, patients recount that painful episodes are often managed at home. The effect of home pain management on activities necessary for normal development, such as attending school, has not been described.
Children with chronic illnesses often miss school. Public policy in many states dictates that homebound instruction is provided to ill students only after a certain consecutive number of school days are missed (Hobbs et al. 1985). The impact of SCD related pain on school attendance and the average consecutive number of days missed has not been delineated. We report data on
3 Home Management of Sickle Cell Pain
the frequency of sickle cell related pain and its effects on school attendance from 18 children and adolescents followed over an average of 10 months each. The data were collected using a home pain diary developed specifically for patients with SCD (Shapiro et al. 1990).
METHODS
Patients
Patients were enrolled in a study of the natural history of sickle cell related pain, and of the efficacy of self-hypnosis as an intervention. Eligibility criteria included (a) diagnosis of a sickle hemoglobinopathy; (b) age between 7 and 17 years; (c) retrospective report of at least four painful episodes over the previous year; and (d) identification of pain as a significant problem by the patient and the family. Exclusion criteria were regular red blood cell transfusion therapy, co-existence of other serious chronic illnesses, mental retardation, and emotional or family problems requiring ongoing psychotherapy.
All patients were followed at the Comprehensive Sickle Cell Center of The Children's Hospital of Philadelphia. Of the 380
4 Home Management of Sickle Cell Pain
patients followed at the Center, 144 were eligible by age and diagnosis, and met no criteria for exclusion. Thirty-three of these patients could not be contacted, and 78 did not have frequent enough painful episodes to meet the eligibility criteria. Nine eligible patients declined to participate, citing reasons such as "could not make appointments" (5); "not interested" (2); and family member did not want the patient to participate (2). Six patients who expressed initial interest could not subsequently be contacted.
The enrolled patients ranged from 8 to 17 years of age (average of 13 years). There were 7 girls and 11 boys; boys and girls did not differ significantly in age. The average length of time that patients stayed in the study was 10 months, with a range of 2 to 15 months.
The Committee for the Protection of Human Subjects at The Children's Hospital of Philadelphia approved the study. Informed consent was obtained from parents and patients before enrollment.
The Home Diary
A pain diary was developed from a self-report system used for research on sleep and circadian rhythms (Shapiro et al. 1990). The
5 Home Management of Sickle Cell Pain
diaries were compact, each 5" by 7", and covering a one week period of time. Patients were asked to complete two pages each day, one in the morning as soon after awakening from sleep as convenient, and one in the evening before going to bed. On the morning page, patients indicated the presence of any SCD related pain by circling "yes" or "no". If "yes" was circled, they indicated the pain intensity on a 10-cm linear analogue scale. Patients also indicated by circling "yes" or "no" whether or not they slept well, and rated their perceived sleep length on a 5-cm linear analogue scale. At night, children were again asked about the presence and intensity of SCD related pain, school attendance on weekdays, and medication use.
The diaries were attractively printed on heavy paper. The cover page was personalized with the child's name, the dates of the week, and the statement that this was a confidential record. On the last page was a statement thanking the child for completing the diary, and reminding the patient to place the diary in the mail.
Procedures
Patients and their families were told that participation in the study involved a responsibility to complete and return the diaries. Possible difficulties in adherence were openly discussed,
6 Home Management of Sickle Cell Pain
and a joint problem solving approach used to define solutions that were compatible with the children's and families' lifestyles and preferences. It was emphasized that responsibility for the diaries should not add stress to daily life, nor should it precipitate conflicts between parents and children. The relative responsibilities of children and their parents were defined, with individual variations based on factors such as developmental maturity and interactional styles. In general, parents helped children under the ages of 10 or 11 remember to complete the diaries, whereas older children were encouraged to develop their own reminder systems. Older teenagers took full responsibility for the entire process.
To facilitate completion and return of the diaries, procedures were instituted that had been used successfully in long term studies of mood (Dinges 1989). Each week a packet containing the diary for the following week and a preaddressed stamped envelope in which to return the diary was mailed to the patient. Two of the authors (BSS and LBR) contacted the families by phone on an average of once every two to three weeks. During these calls, we discussed the entries in the diaries that we had received, provided positive reinforcement and reminders when necessary, and elicited concerns and questions about pain management and study
7 Home Management of Sickle Cell Pain
interventions. If less than 25% of the diaries were returned for 2 months in a row, the patients and families were asked whether they still wished to be in the study. If further participation was declined, the patients were dropped from enrollment.
We discovered early in the study that patients who otherwise adhered to the protocol did not complete the diaries when they were hospitalized. Therefore, the diary data pertain only to home management. However, because we followed the patients closely, we knew when and why they were hospitalized. Therefore, the data include the number and timing of pain days spent in the hospital. These data were used along with the diary data to assess the relative rates of home versus hospital management, the proportion of days with pain, and the duration and number of painful episodes.
Analysis of Data
Adherence to the study protocol was determined from the number of diaries completed and returned; including time spent in the hospital. Pain was evaluated both as the proportion of days that pain was reported out of the sum of the total number of diary days completed plus hospital pain days, as well as by the total number of painful episodes managed at home, in the hospital, or both
8 Home Management of Sickle Cell Pain
(i.e., each discrete multi-day period of pain). To evaluate the effects of pain on outcome variables, each patient's home diary data was reduced according to report of the presence or absence of pain. With this system, each patient generates only one data value, regardless of the amount of time in the study. Thus, for each diary dependent variable (e.g., sleep quality), data were averaged within all days in which pain was not reported and separately within all days in which pain was reported. For each dependent variable, "pain" and "no pain" distributions were examined for homogeneity of variance. Violations resulted in use of nonparametric statistical comparisons. Mann Whitney U statistic was used to compare pain patterns of male and female patients. Wilcoxon matched pairs signed ranks tests were used to evaluate differences in sleep and school attendance between days with and without pain. Spearman rank order correlations were used for assessing the relationship between age and pain. Analyses were conducted including and excluding a 14-yr old female patient who reported pain virtually every day (case #16 in Table 1). Those instances in which her exclusion changed the findings are reported in the results. Outcomes were considered statistically significant if p< .05, two-tailed.
9 Home Management of Sickle Cell Pain
RESULTS
Adherence with the Daily Diaries
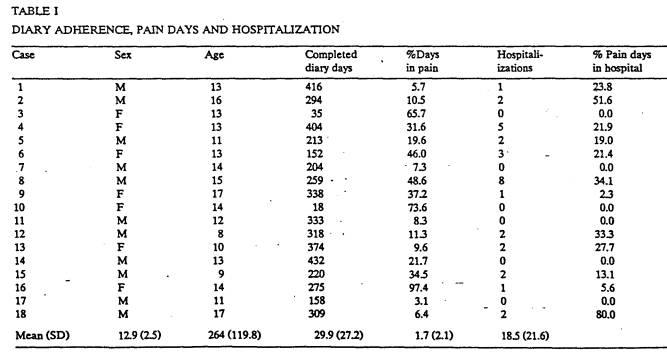
A total of 4,756 completed diary days were received from the 18 patients. Patients completed an average of 264 diary days each, although there was considerable inter-subject variability (Table 1). On average, 75% of the diary days were completed each month. Adherence to the diary system was inversely related to the percentage of days on which painful episodes were reported (r = - 0.658, p < 0.01), and was not related to age, sex, the number or intensity of the painful episodes, or the absolute number of completed diary days. Adherence with the diaries gradually declined over the first 10 months of enrollment. Average adherence was 90% in the first month and 63% in the tenth month, giving an average decrease of 2.7% each month.
___________________
Insert Table 1 about here
___________________
10 Home Management of Sickle Cell Pain
Home Versus Hospital Management of Pain
If any part of a painful episode involved emergency department or inpatient hospitalization, this episode was considered to have been managed in the hospital. Pain was managed entirely at home during 89% of the painful episodes (81% of the days with pain). However, patients varied widely in hospital contact for pain management (Table 1). Six patients had no hospitalizations for pain. The remainder were hospitalized for an average of 16% of painful episodes (SD=13.73; range 4% - 50%). Comparisons of these two subgroups revealed few significant differences. Hospitalized children reported a greater number of painful episodes (M = 24.2, SD = 15.7) than did non-hospitalized children (M = 10.6, SD = 10.8; U = 13, chi 2 = 4.08, df = 1, p = < .05). However groups did not differ in the proportion of days with pain, (hospitalized M = 23.7, SD = 16.2; non-hospitalized M = 29.9, SD = 31.5), in the intensity of pain managed at home and reported in the diary, or in demographic or activity (e.g., school attendance, sleep) variables.
Age Related Patterns
The patterns of the painful episodes varied greatly among patients. Pain was reported on an average of 30% of all days (26%
11 Home Management of Sickle Cell Pain
with the exclusion of patient # 16; see Table 1), with a range of 3% to 97% (median = 20.7%). On average, two episodes of pain were reported each month (range 0 - 5), with a mean duration of approximately 4 days (range 1 - 17 days). Analog pain intensity ratings (0 = none; 100 = the worst) during painful episodes managed at home averaged 29, with a range from 10 to 69.
Age was examined in relation to the percentage of days with pain and the frequency, length, and average intensity of painful episodes. Older patients reported longer painful episodes (rho = .677; t = 3.67; p < .01). There was no relationship between age and the frequency or intensity of pain, or the number of painful episodes.
Sleep Patterns
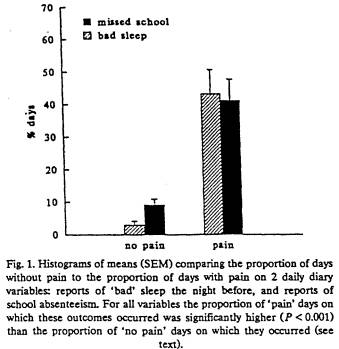
Ratings of sleep quantity and quality were influenced by pain. Patients reported poor sleep on an average of 43% of days with pain (SD = 32%), compared to only 3% of days without pain (z = 3.57; p < .001; Figure 1). Similarly, reported sleep duration was significantly less on nights in which pain occurred relative to nights without pain (z = 3.62; p < .001).
12 Home Management of Sickle Cell Pain
___________________
Insert Figure 1 about here
___________________
Effect of Pain on School Attendance
3,186 potential school days were analyzed. (Days were counted as potential school days when a daily diary report was available or when patients were hospitalized for pain management and school was in session. Days for which there were no diary data and days during which patients were hospitalized for problems not related to pain were excluded.) Patients missed school on 41% (SD = 27.8%) of the days on which they reported pain, compared to an average of 9% (SD = 7.3%) on days without pain (z = -3.29; p < .001; Figure 1). Of all missed school days, about half (11% of all potential school days, with a range of 0 - 40%) were on days with reported painful episodes. There was no significant difference between the rate of missed school on the day after a painful episode (when patients might be expected to be recovering) and on other pain-free days. Of the school days missed because of painful episodes, 65% were missed when pain was managed at home, and 35% were missed when pain
13 Home Management of Sickle Cell Pain
was managed in the hospital.
Correlational analysis showed a significant relationship between missing school on days with and on days without pain (rho =.523; t = 2.37; df = 15; p < .05). The average pain intensity per month was correlated with school absence on days with pain (rho = .599; t = 2.99; df = 16; p < .01), and with school absence on days without painful episodes (rho = .482; t = 2.13; df = 15; p < .05). The average analog pain score when school was missed because of pain managed at home was 55 out of 100 (range 8 - 86), relative to a significantly lower pain score of 30 (range 15 - 47) when school was not missed. There were no relationships between the rate of school absence on days with or without pain and the percentage of days with pain, sleep quality, adherence to the diary system, or the rate of hospitalization.
Even though the children missed an average of 6 to 8 weeks of school within a school year, the average consecutive number of days on which school was missed was 2.7, with a range of averages of 1-9.
14 Home Management of Sickle Cell Pain
DISCUSSION
Patient selection
Patterns of interaction with the health care system vary widely among patients with frequent pain and their families. Many families regularly participate in outpatient follow-up, including medical, educational, mental health, and supportive services (outpatient based management). Other families more often interact with health care professionals at the time of hospitalization (hospital based management) (Shapiro 1993).
Families and patients who espouse outpatient based management may have been more likely to participate in this study. We were unable to compare factors which could have influenced participation (e.g., socioeconomic status, family function, social supports, health care beliefs) between families choosing and not choosing to enroll. Additionally, the total number of patients enrolled and studied is small. Therefore, the results must be interpreted as preliminary, and not necessarily representative of all patients with frequent painful episodes. However, patients with frequent and severe pain who rely on hospital-based management are unlikely to experience less impact of the pain on activities of daily living.
15 Home Management of Sickle Cell Pain
Adherence
Adherence to the diary system and the study was extremely high, especially considering the nature of the task and the longterm enrollment. There were limitations, however, to determining adherence. Although we could ascertain whether or not the diaries were completed and returned, we do not know whether they were filled out twice a day as instructed, or whether the entire diary was filled out at one time before return. Therefore the results must be understood as an approximation of the pain experience.
Several factors may have facilitated adherence. Patients were self-selected, and their electing to participate in such a study evidenced beliefs in the value of anticipatory, non crisisoriented intervention. The study design included methods to enhance adherence (Shapiro et al. 1990). Finally, even though we presented the diaries as a way of helping us understand the pain, many patients and families viewed the diaries as therapeutic, perceiving a benefit to themselves in recording pain and examining patterns.
We expected that pain would motivate patients to maintain participation. However, patients with more pain days had lower rates of diary completion. This result could reflect the complex
16 Home Management of Sickle Cell Pain
interrelationships among pain perception, coping styles, family organization, attributional style, and mood.
Home versus Hospital Management
The vast majority of painful episodes were managed entirely at home. Coming to the hospital for pain management likely reflects complex interactions among such factors as pain intensity, learned behaviors, coping styles, external stresses and supports, and health care beliefs of the patient and the family.
Although the number of hospitalizations may be a sensitive indicator of illness severity for patients who tend to come to the hospital, there appears to be a group of patients for whom the rate of hospitalization does not indicate the extent and impact of the pain. If we aim to understand and reduce the impact of pain on psychosocial function and quality of life, we must include pain that is managed at home in our studies of assessment and intervention, as well as in our clinical approach to patients. The frequency of pain is an important criterion in selecting patients for treatment outcome studies. Our data suggest that in such studies the evaluation of treatment outcome may be inaccurate unless a system to track pain managed at home is included. Additionally, the fact that nearly 90% of painful episodes were
17 Home Management of Sickle Cell Pain
managed at home in this group of patients highlights the need for programs designed to help children and families to manage their pain.
Pain Patterns
The patients in this study experienced pain on a surprisingly high number of days. Clinicians often regard sickle cell related pain as being an acute or acute recurrent pain syndrome. However, patients with frequent painful episodes are more accurately designated as having chronic or chronically recurrent pain. Since the clinical approaches to patients with chronic and acute pain differ, recognition of the pervasiveness of pain in everyday life is key.
These data were obtained during the course of an ongoing interventional study utilizing self-hypnosis and education. These interventions, which were started about 4 months into the study, may have affected the actual or reported frequency, intensity, and/or duration of pain. However, these aspects of the pain experiences are unlikely to have been increased by the interventions. Therefore, the data reported here may actually underestimate the impact of pain.
18 Home Management of Sickle Cell Pain
Sleep Patterns
The effects of pain on sleep quality and duration were profound. Since poor or inadequate sleep may affect pain coping during the day, as well as attentiveness at school, this relationship is clinically significant. Pharmacologic and nonpharmacologic interventions targeting sleep may augment daytime performance.
Effect of Pain on School Attendance
This particular group of patients missed about one fifth of their school days. Only half of those absences were associated with SCD related pain. The absences on days without vaso-occlusive pain could have a number of causes, including minor infections, clinic visits, or other medical problems associated with SCD. The impact of pain and illness on psychosocial function could also affect school attendance. Families may perceive their children as vulnerable, and keep them out of school for problems that would not interfere with school attendance for most children. Additionally, falling behind in schoolwork may develop into a pattern of school avoidance. Our finding of a relationship between the proportion of school days missed on days with and days without pain is consistent with these possibilities.
19 Home Management of Sickle Cell Pain
Home management of pain is often encouraged by health care professionals as a way to normalize everyday functioning. However, children with frequent pain and infrequent hospitalizations may be at significant risk of school absenteeism. Although the relationship between absenteeism and school performance has not been studied in these children, we can assume that frequent absences are likely to lead to problems. These children may be overlooked for intervention because, unlike children who are frequently hospitalized, the extent of dysfunction may not come to the attention of health care professionals.
Although these children missed an average of 6 to 8 weeks of school each year, they missed on average less than 3 consecutive days at a time. Thus, they do not qualify for help in states that require 1 to 2 weeks of consecutive missed school days for homebound tutoring, and even in states that provide more immediate homebound assistance, by the time the paperwork is filed and processed the child is ready to return to school.
Further work is necessary to delineate the impact of these absences on school performance and psychosocial status, and to develop cost effective and pragmatic ways of providing adequate educational opportunities for children and adolescents with sickle cell disease.
20 Home Management of Sickle Cell Pain
21 Home Management of Sickle Cell Pain
22 Home Management of Sickle Cell Pain
Figure Caption
Figure 1. Histograms of means (SEMs) comparing the proportion of days without pain to the proportion of days with pain on two daily diary variables: reports of "bad" sleep the night before, and reports of school absenteeism. For all variables the proportion of "pain" days on which these outcomes occurred was significantly higher (p < .001) than the proportion of "no pain" days on which they occurred (see text).
23 Home Management of Sickle Cell Pain
REFERENCES
Dinges, D.F., Napping patterns and effects in human adults. In: D.F. Dinges, and R.J. Broughton (Eds.), Sleep and Alertness: Chronobiological, Behavioral and Medical Aspects of Napping, Raven Press, New York, 1989, pp. 171-204.
Hobbs, N., Perrin, J., and Irey, H., Chronically ill children and their families, Jossey-Bass, San Francisco, 1985.
Platt, O., Thorington, B.D., and Brambilla, D.J., Pain in sickle cell disease: rates and risk factors, N Engl J Med, 325(1991)11-16.
Samuels-Reid, J., and Scott, R.B., Painful crises and menstruation in sickle cell disease, South Med J, 78(1985)384-385.
Serjeant, G.R., Sickle Cell Disease, Oxford University Press, Oxford, 1985.
Shapiro, B., Management of painful episodes in sickle cell disease. In: N.L. Schechter, C.B. Berde, and M. Yaster (Eds.), Pain in. Infants, Children, and Adolescents, Williams and Wilkins, Baltimore, 1993.
Shapiro, B., Dinges, D.F., and Orne, E.D., Recording of crisis pain in sickle cell disease. In: D. Tyler, and E. Krane (Eds.), Advances in Pain Research and Therapy, Raven Press, New York, 15(1990)313-321.
Tetrault, S.M., and Scott, R.B., Five year retrospect study on hospitalization and treatment of sickle cell anemia patient. In: Proceedings of the First National Symposium on Sickle Cell Disease, Bethesda, 1974.
Vichinsky, E.P., Johnson, R., and Lubin, B.H., Multidisciplinary approach to
pain management in sickle cell disease, Am J Peliatr Hematol Oncol, 4(1982)328-333.
See also the Pain Homepage at http://www.sciencedirect.com/science/journal/03043959